The correlations of serum to CSF concentrations of the measured steroid hormones (DHEA, E2, P4) vary according to the specific steroid in our cohort of 27 women at term pregnancy. Our results for pregnant women are consistent with the repeated observation in non-pregnant subjects, that steroid concentrations broadly differ at least by one to two orders of magnitude between the serum to CNS compartments (23, 24). We found the strongest inter-compartment correlation for DHEA. On the contrary, correlations for estradiol were rather weak, and for progesterone weak but significant. Interestingly central E2 concentration correlated best to serum DHEA (moderate correlation) and to central DHEA (strong correlation).
To our knowledge this is the first study observing CSF to serum concentrations of neuroactive steroid hormones in women at term pregnancy. CSF and serum concentrations were measured from simultaneously collected samples. Robust correlation effects could be shown over a wide range of the hormone serum concentrations that are typically found in pregnancy. We choose a set of steroids with neuroactive potential that are most available in clinical routine analysis. A second and more important reason for measuring estradiol and progesterone is that these are the two most discussed neuroactive steroids in seizure susceptibility in women with epilepsy (4).
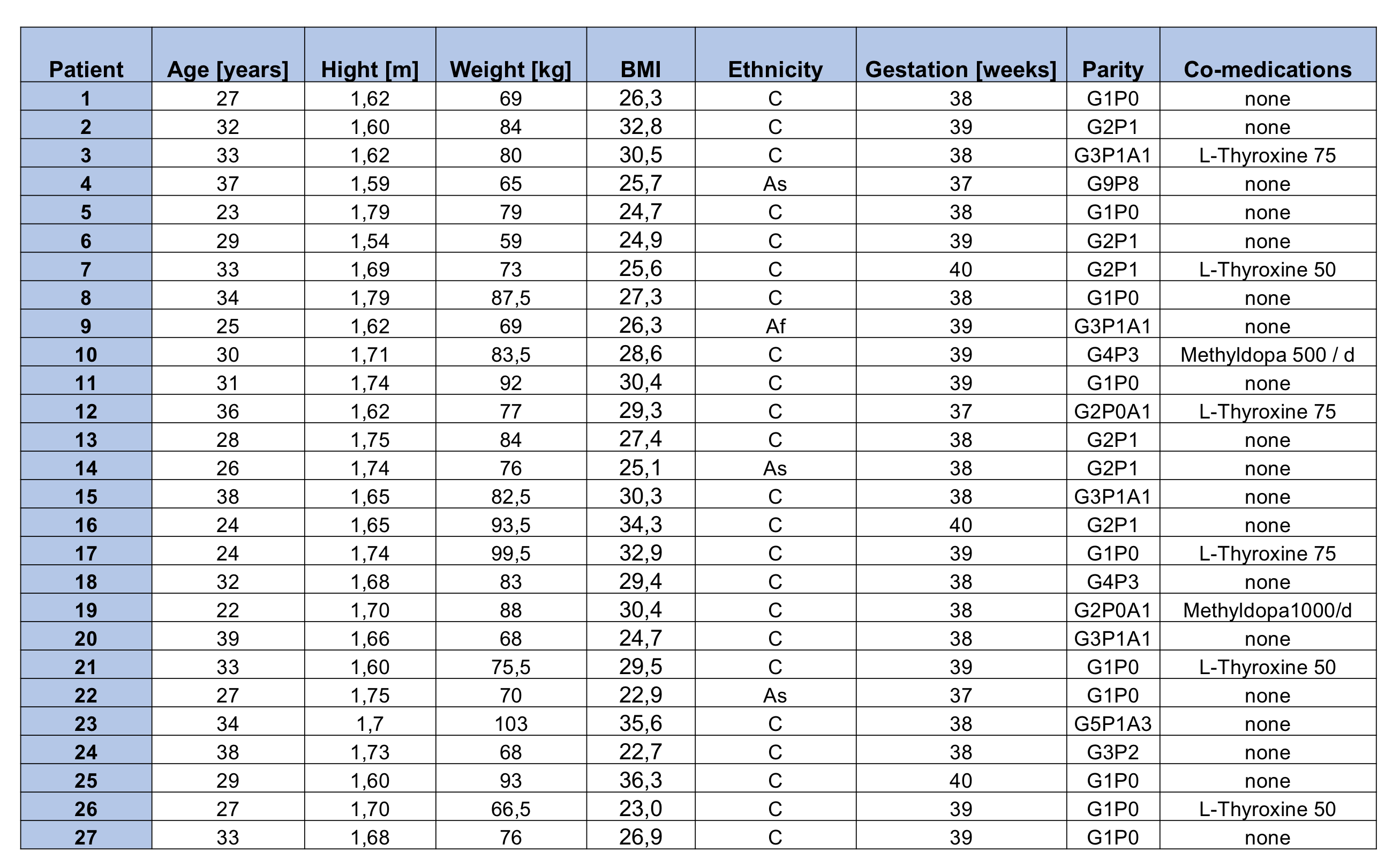
Pregnancy is a distinct physiological condition that might include changes in blood-brain-barrier function as well as central and peripheral steroid metabolism compared to non-pregnant subjects. Therefor the results may not be valuable for non-pregnant women and men. Our study population of 27 subjects was small, though comparatively large regarding published populations in this field. Statistical evidence base is limited due to a small sample size. ElISA were not constructed for hormone analysis in CSF (25) Mass spectrometry might be superior for precise steroid detection in CSF, but was not available for this study.
The transformation from cholesterol to progesterone or DHEA and further from DHEA via the down-stream androgenes androstendione and testosterone towards their aromatization to the estrogenes estron and estradiol (E2) are major human steroidogenic pathways (26). The main serum availability of these steroids in premenopausal women derives from peripheral glands (ovaries, adrenals) and in case of pregnancy from the fetoplacental unit. Extraordinarily high circulating E2 concentrations during pregnancy result from placental aromatase activity. The placental steroid production exceeds physiologic concentrations in non-pregnant women by several orders of magnitude. Estradiol serum concentrations rise 100 to 500-fold during pregnancy, compared to normal cycle conditions (27).
Steroid hormones cross the blood brain barrier to a certain extent, but the intercompartment equilibrium between serum, CSF and neural tissue is unclear (10). In line with our results, in vivo data of patients, though scarce in number, suggest that the steroidal environment in CNS versus intravascular compartments differs by a magnitude of 10 to 100 with lower concentrations in the CNS. Animal models support these findings (10, 28). CNS tissue concentrations are not necessarily reflected in CSF (23). Most stable correlations were found for DHEA in CSF and temporal brain tissue (29). The study of intra-tissue steroid hormone formation and metabolism (intracrinology) reveals the expression of required enzymes for steroid hormone synthesis in topical variance in the brain tissue, although there are conflicting data concerning the complete steroid biosynthetic pathways in human CNS (30). The balance between intra tissue de novo synthesis to systemic delivery of hormone precursors or ready for function steroid effectors has not yet been disentangled.
In conclusion of these findings and our data central E2 seems to originate mainly from local synthesis based on local or peripheral DHEA supply as a precursor hormone to estrogen after aromatization. In this regard peripheral DHEA can be interpreted as a predictor of central E2, whereas our data suggest a at least a partial peripheral to central P4 transport. A DHEA to P4 ratio from serum hormone concentrations would allow a prediction of the E2 to P4 ratio in a central compartment.
Since estradiol is a potentially proconvulsive neuroactive steroid, and progesterone has a tendency to have a depressant effect, a proportional increase of estradiol compared to progesterone concentration in the CSF in the course of pregnancy would result in an excitatory neurosteroidal environment due to overweighing neuroactive estradiol effects.
In most women with epilepsy (WWE) the status quo of seizure frequency appears to remain controlled during pregnancy. But studies report an increase in seizure frequency for 20-50 percent of WWE during pregnancy (31-34). A reliable predictor has not been identified yet. In an attempt to exclude anti-epileptic drugs (AED) serum concentration dependent effects such as accelerated metabolism in pregnancy or incompliance to medication intake Vajda et al. still found a significant rise in seizure frequency in a Australian pregnancy register based case series of women with medically untreated epilepsy during pregnancy (35).
Neuroactive hormone balance signatures are not systematically examined or reflected as predictors of seizure frequency worsening in pregnant WWE. A pregnancy is an exceptional endocrine situation with excessive hormone synthesis and highly variable serum concentrations compared to normal cyclic conditions. The clinically observed increase of seizures in patients without AED may partly be influenced by rising estradiol to progesterone ratios in the CNS. The predictive potential of peripheral DHEA concentrations as a surrogate marker for central E2 concentrations might identify patients at risk for seizure e.g. from epilepsy or preeclampsia due to endocrine CNS modulation.
Therefore, clinical observation with clear concomitant measurement of neuroactive hormonal distribution is required. Here, we offer a clinical tool (peripheral DHEA/P4 ratio to calculate CSF E2/P4 ratio) that allows predictive insight of neuroactive steroid concentrations in a CNS compartment from the easily accessible peripheral serum compartment.
{kind=link}