Patients characteristics
Of the 2162 individuals scheduled to attend their out-patient appointments between 1st January 2019 and 31st August 2019 at the clinics in both QMH and RTSKH (1962 from QMH and 200 from RTSKH respectively), 27 fulfilled the inclusion criteria and 14 of them agreed to be interviewed (Figure 1). The caregivers of 10 out of 14 patients agreed to be interviewed and they were interviewed as a pair.
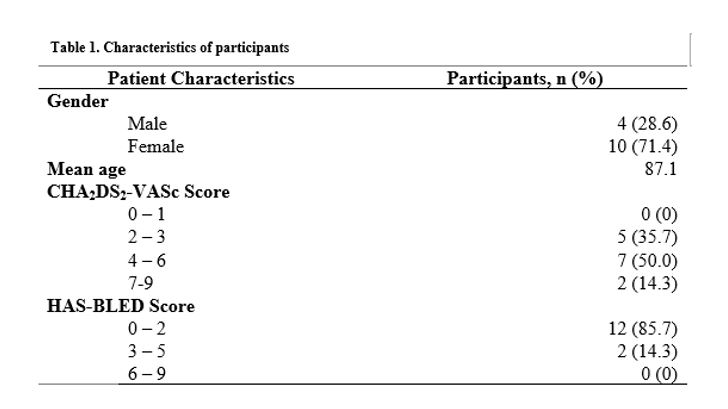
All patients had a CHA2DS2-VASc score of ≥ 2 and 85.7% of them had a HAS-BLED score between 0 and 2. The characteristics of patients are summarized in Table 1. Data saturation was reached after interviewing 14 patients. The interviews lasted approximately 15 minutes.
Five meta-themes were developed: Awareness of AF symptoms and diagnosis; Knowledge and understanding of AF and stroke prevention therapy; Role of decision-making in prescribing; Willingness to switch from aspirin to OACs; and Impact of OACs on daily lives.
Theme 1: Awareness of AF symptoms and diagnosis
More than half of the patients and their caregivers were not aware of symptoms of AF until they were incidentally diagnosed during routine examinations or when complications of AF happened. (“I couldn’t tell if my heart actually beats irregularly but doctor found out after ECG.” P10;“We realized that Grandma got AF after stroke, and she did not take any medications before.” Caregiver of P06). The remaining patients did not recall the fact they had been medically diagnosed with AF.
Theme 2: Knowledge and understanding of AF and stroke prevention therapy
i. Understanding of AF and complications
The majority of the patients had a poor understanding of AF and its complications. They were able to describe AF as having an irregular heartbeat and palpitations without knowing the name of the disease. (“I don’t know the name (AF). The doctor only told me my heartbeat is not good every time.” P12; “What I know from the doctor is heart rhythm is not regular and fast heartbeat.” Caregiver of P07). Some patients and their caregivers also mentioned they could not recall what they had been told by the doctors as doctors might not discuss patients’ heart conditions at every consultation. Only three patients knew that AF increases the risk of having a stroke.
ii. Understanding the importance of stroke prevention
Understanding the importance of stroke prevention therapy is an important facilitator of using OACs. Less than half of the patients and their caregivers could clearly explain that aspirin prevents stroke by reducing the formation of blood clots which cause blockage of blood vessels. However, some patients did not know why aspirin was prescribed and some even had an incorrect understanding of the reasons for taking aspirin regarding to AF. (“Aspirin is used to make the blood become thicker and I’ll be less likely to bleed.” P13; “Aspirin is to slow down the heart rate.” Caregiver of P07).
Furthermore, most patients and caregivers described aspirin as a “blood thinning agent” but they had no knowledge of other OACs available on the market. (“Yes, I only know aspirin. I’m not sure about others (anticoagulants) so I didn’t ask the doctor.”P05). Only the caregiver of one patient was able to illustrate a good understanding of the illness, the importance of stroke prevention therapy, and the difference between OACs and aspirin.
Theme 3: Role of decision-making in prescribing
i. Involvement in discussions with doctors
Patients and caregivers assumed a passive role when communicating with doctors. Generally, there was minimal or no patient involvement in treatment decisions. Most of the time the decisions regarding treatment were made by the doctors and patients accepted their decisions. (“The doctor only told us Grandma has AF and also hypertension so he prescribed aspirin.” Caregiver of P08; “Doctor didn’t say anything but just prescribed aspirin.”Caregiver of P02). A few mentioned that insufficient medical knowledge is also a barrier to determine which treatment option is more suitable for patients. As mentioned above, most patients had no knowledge of other OACs apart from aspirin. This restricted them from contributing to a treatment decision with doctors. (“Doctor can decide and I don’t know much on this (medication), as long as it’s good to Grandma.” Caregiver of P09). The caregiver of one patient mentioned that it was difficult to have an in-depth discussion with the doctors due to limited consultation time. (“Consultation time is very short at the hospital. The doctor will only call you unless there’s something urgent.”Caregiver of P02).
ii. Delegating trust to their doctors
Patients trusted their doctors to decide what medications should be prescribed for their condition because of their professional knowledge and judgement. (“I don’t know what doctor prescribed. I trust the doctor!” Caregiver of P04; “I trust the doctor… I don’t know the medication and I assume the doctor is confident to prescribe the right medication to my Mum. Is that right? Then I trust the doctor.” Caregiver of P11).
Theme 4: Willingness to switch from aspirin to OACs
i. Fear of adverse effects from OACs
Patients and caregivers expressed their concerns of the adverse effects of OACs compared to aspirin, predominantly the risk of bleeding. They were particularly concerned about potential bleeding complications and fearful about what might happen, leading to them to reject OACs. (“I dare not take it (OAC). I don’t want to take it. It will cause non-stop bleeding! I’m scared!” P10). Due to the fragility of elderly patients, their caregivers were worried that the potential of bleeding easily from OACs would increase risk of injuries and hence adversely impact patients’ quality of life. (“We need to consider if we let Mum take it (OAC) or not. My mum always scratches herself and bleeds easily. The doctor told me about the problem of bleeding. I’m afraid the wounds will get inflamed easily…… Also, if she falls at home, it takes a long time for the bruises to disappear.” Caregiver of P02; “I’m worried that if the ‘blood thinning’ of OAC is stronger than aspirin, Mum will faint easily. I don’t agree taking OAC.”Caregiver of P03)
ii. Risk assessment of aspirin and OACs
Most patients and their caregivers perceived that aspirin is a suitable medication for them if they do not experience any adverse effects or find them manageable. (“I’m fine with taking aspirin so I won’t consider changing to another new one.” P10) For older patients, their caregivers expressed concerns that it would be difficult for older people to adapt to new medications including dosing regimen, lifestyle modifications and most importantly, the tolerability of unknown adverse effects. Therefore, most patients and caregivers felt the risks of experiencing any unknown adverse effects that they might be unable to tolerate outweighed the risk of having a stroke. (“Since Mum is old, her body function starts to deteriorate slowly. If the doctor always changes her medication, I’m afraid she won’t be able to adapt” Caregiver of P04). Only the caregiver of one patient placed more value on the benefits of stroke prevention of OACs and would consider switching from aspirin to OAC in the future.
Theme 5: Impact of OAC regimen on daily living
Patients and caregivers believed that the initiation of OACs would be inconvenient in their day-to-day lives. Compared to aspirin, the regimens of OACs are more complicated, in which regular drug monitoring, diet restrictions and occasional adjustment of dosage would be required. (“The doctor was planning to prescribe warfarin but……. Grandma will need to do blood tests every few days and then adjust the dose again. She is pretty old now so aspirin is much simpler. It’s better for her……… Also, she doesn’t need to avoid eating some of the food for aspirin but warfarin.”Caregiver of P04) One patient experienced gastrointestinal bleeding after taking NOAC, hence aspirin was prescribed after the cessation of NOAC.
{kind=link}