Fifty-four consecutive patients were seen for biliary tract diseases. Of these, 13 patients met the following exclusion criteria and were excluded from the analysis. Finally, 30 BTC patients and 11 BBD patients were included. Ten healthy, age-matched subjects were also recruited for faecal microbiota comparison (Figure 1). All patients with biliary tract disease and controls were recruited at Jikei University Kashiwa Hospital. The diagnosis of BTC was based on cholangiography, the presence of typical cholangial lesions on tissue biopsy (if possible), contrast CT findings and elevated tumour markers. The exclusion criteria were patient age less than 18 years, acute bacterial cholangitis, severe medical comorbidities, and previous receipt of treatment interventions, such as endoscopic retrograde cholangiography (ERC) and surgical or anticancer therapy. Patients had to not receive antibiotics within two months prior to participation in the study. This interval was determined to be a sufficient period of time for the gut microbiota to recover from the effects of antibiotic administration. To reduce the effects of geographic conditions, genetic background and diet, all recruited participants were Japanese and had lived in the Kanto region for a number of years.
Indications for ERC in patients with BTC included the purpose of bile stasis treatment or BTC diagnosis; during ERC, bile aspiration was performed without the use of contrast or interventional antibiotic prophylaxis. No patients with BTC were sampled for acute suppurative cholangitis. The BBD group was established as controls and included those with surgical intent for gallbladder stones or gallbladder polyps. Patients with chronic cholecystitis or acute cholecystitis, a condition that produces persistent inflammation, were excluded. All subjects provided written informed consent, and the study was approved by the clinical research ethics committee of the Jikei University School of Medicine and Kashiwa Hospital, Tokyo Jikei University School of Medicine (number 29-146 (8762)). This study was conducted in accordance with the Declaration of Helsinki.
Analysis of the faecal microbiota
Faeces were collected on the morning of the hospital visit, and a stool sample aliquot was mixed with 1 ml of guanidine thiocyanate (GuSCN) solution (TechnoSuruga Laboratory Co., Ltd., Shizuoka, Japan), immediately frozen at -80°C and stored until analysis. DNA extraction from the human faecal samples was performed using the bead-beating method as previously described, with some modifications[14]. Briefly, 150 μl of faecal sample in GuSCN solution was vigorously vortexed with 300 mg of glass beads (AS ONE BZ-01) and 500 μl of Tris-EDTA (TE, pH 9.0) buffer-saturated phenol (Fujifilm, Wako Pure Chemicals) using a FastPrep-24 (Funakoshi Corporation) for 30 seconds at power level 5. After centrifugation at 10,000×g for 10 min, 400 μl of the supernatant was extracted with 500 μl of phenol-chloroform, and 250 μl of the supernatant was precipitated with isopropanol. The purified DNA was suspended in 100 μl of TE buffer (pH 8.0).
Bile collection procedure and biological sample acquisition
Bile was collected during endoscopic or surgical treatment. Bile samples were collected in Techno Suruga Lab containers as in the faecal microbiota analysis. Some bile was also cultured simultaneously with the culture method using the medium described below. All endoscopic surgeries were performed under conscious sedation. Endoscopic retrograde cholangiography was performed with a standard video duodenoscope (TFJ 260-V, Olympus, Tokyo, Japan). A Cook cannula (Cook, Washington, USA) and a Boston guidewire (Boston Scientific, Tokyo, Japan) were used for selective cannulation of the bile duct. A bile sample was aspirated prior to the application of the contrast agent. Antibiotic prophylaxis was applied intravenously after bile samples were obtained and endoscopic scrutiny and treatment were completed. All cholecystectomies or BTC surgeries were performed under general anaesthesia, either open or laparoscopic. Bile samples were aspirated and collected by aseptic manipulation. The biological samples were stored immediately after sampling at -80°C until DNA extraction.
Bile culture assay
Bile was collected intraoperatively by sterilization from consenting patients with BTC or BBD who underwent surgery. A part of the bile was cultured immediately. For anaerobic culture, bile was collected in Kenky Porter II (KP-C0402, Terumo Co., Ltd.), inoculated with 100 μl of Kenky Porter II in the following medium and incubated anaerobically for 48 h. The resulting colonies were collected, and DNA was extracted. Sheep blood agar medium (E-MP35, Eiken Chemical), GAM agar medium (05420, Nissui), gentamicin (20 μg/ml) (Sigma, G1272)-supplemented GAM agar medium, and FM agar medium (05441, Nissui) were used. For aerobic culture, bile was collected in a stool collection container (Technosulga Lab) for intestinal microbiota testing, inoculated with 100 μl of sheep blood agar medium (Eiken Chemical Co., Ltd.) and BTB agar medium (E-MA84, Eiken Chemical Co., Ltd.) and incubated aerobically for 24 h. DNA was extracted from the mixed colonies in each sample.
Microbiota analysis
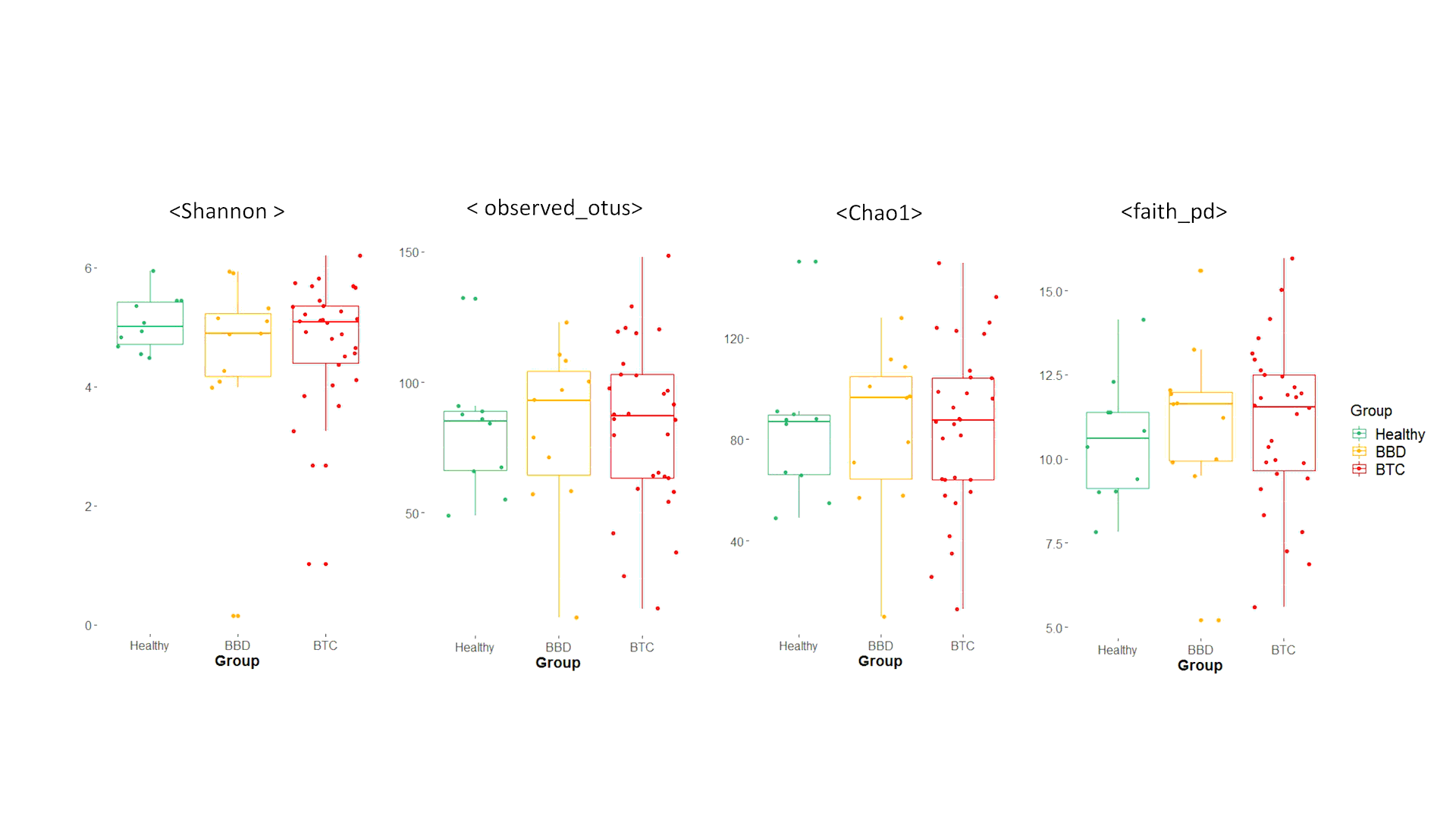
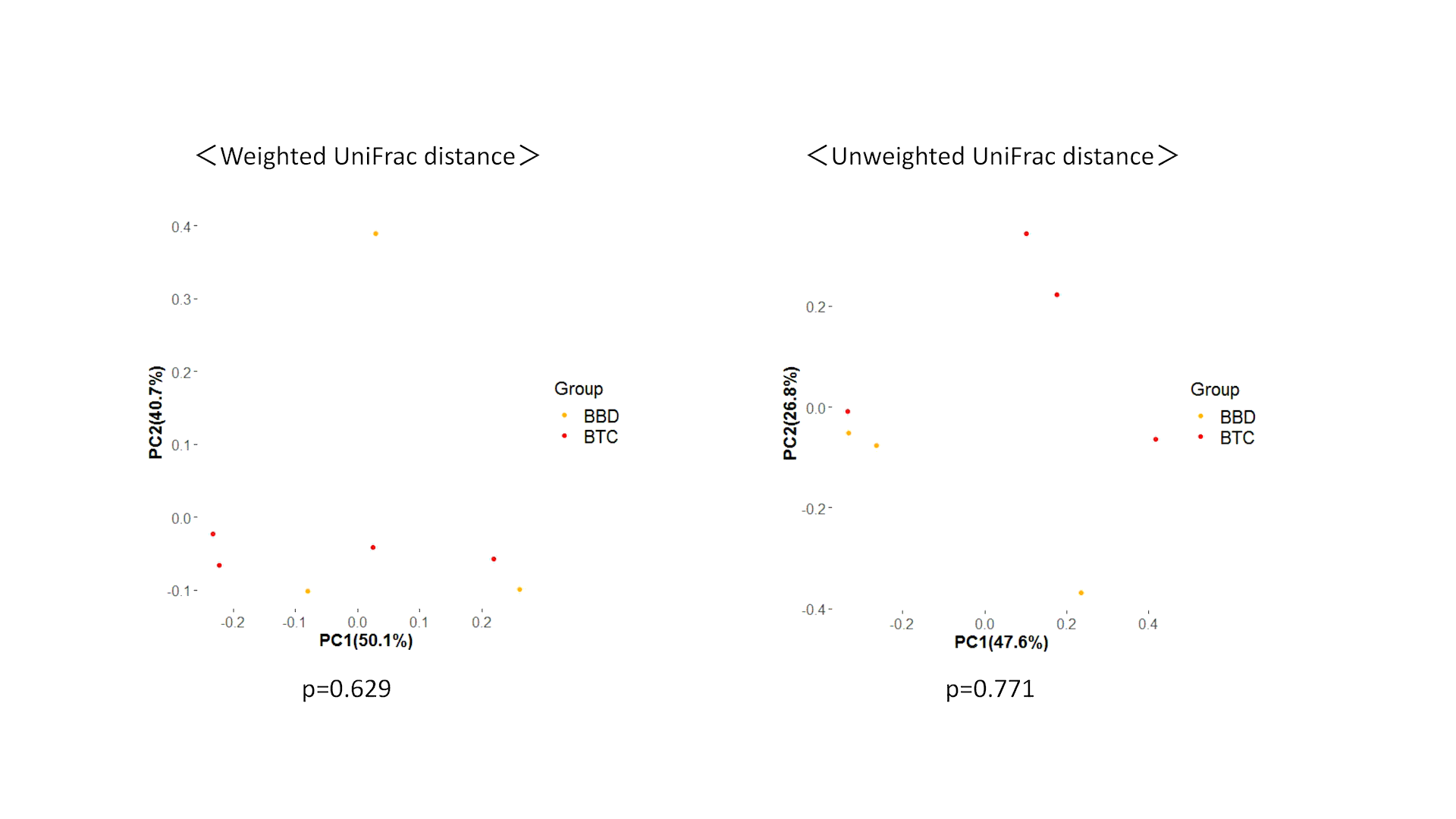
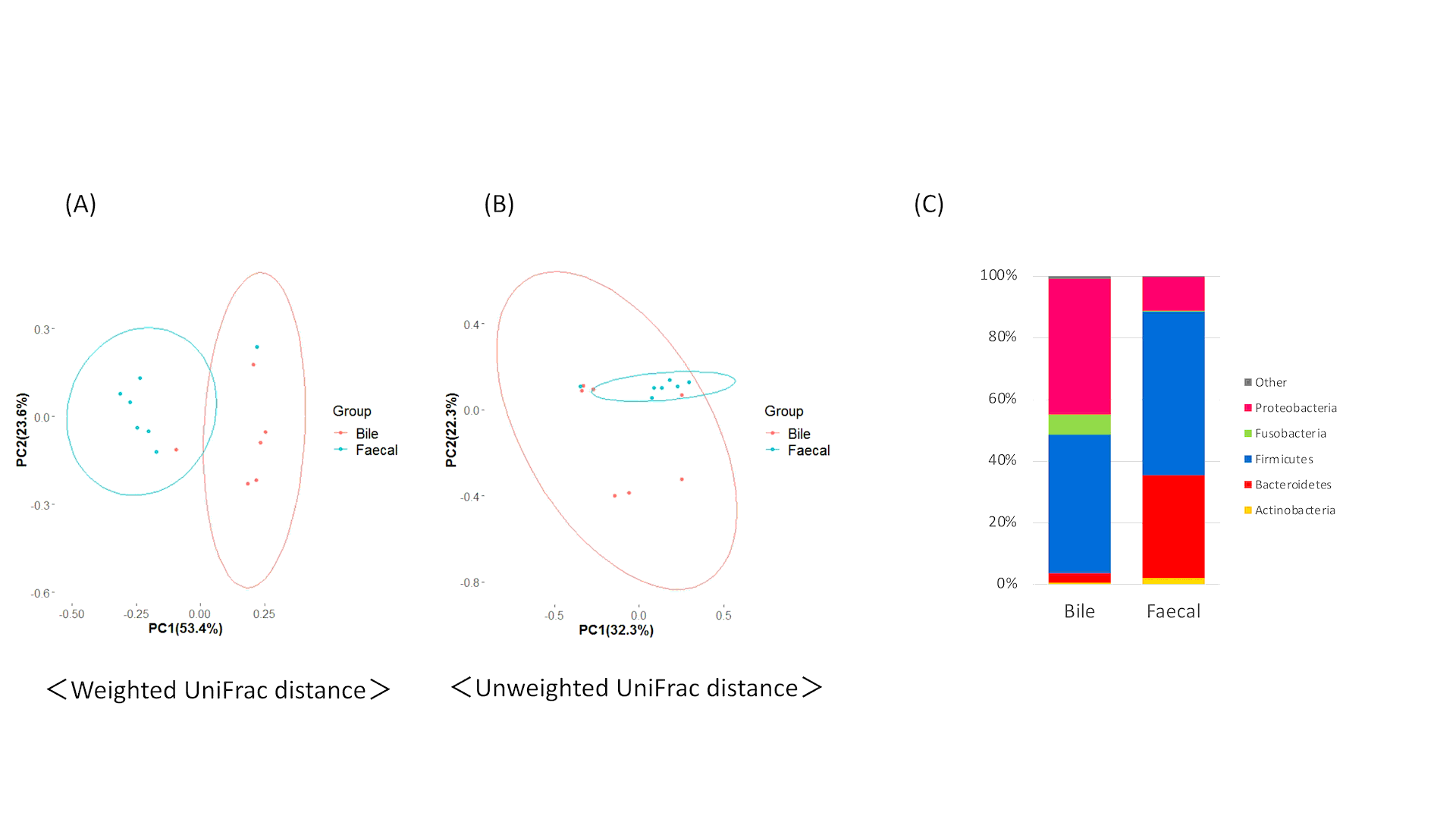
Amplicon sequencing of the V3-V4 regions of the bacterial 16S rRNA gene was performed with an Illumina MiSeq instrument, as described previously[14]. Data were analysed in the QIIME2 software package[15] (ver. 2017.10). The reads were mapped to the PhiX 174 sequence and the Genome Reference Consortium human build 38 (GRCh38) by the Bowtie-2 program[16] (ver. 2–2.2.4), and potential chimaeric sequences were removed from acquiring the Illumina paired-end reads by using DADA2[17]. Thereafter, 30 and 90 bases of the 3′ region of the forward and reverse reads were trimmed, respectively. Taxonomic classification was performed using a naive Bayes classifier trained on Greengenes 13.8[18], with a 99% threshold for operational taxonomic unit (OTU) full-length sequences. Estimation of alpha diversity and principal coordinate analysis (PCoA) for beta diversity were also performed using QIIME2.
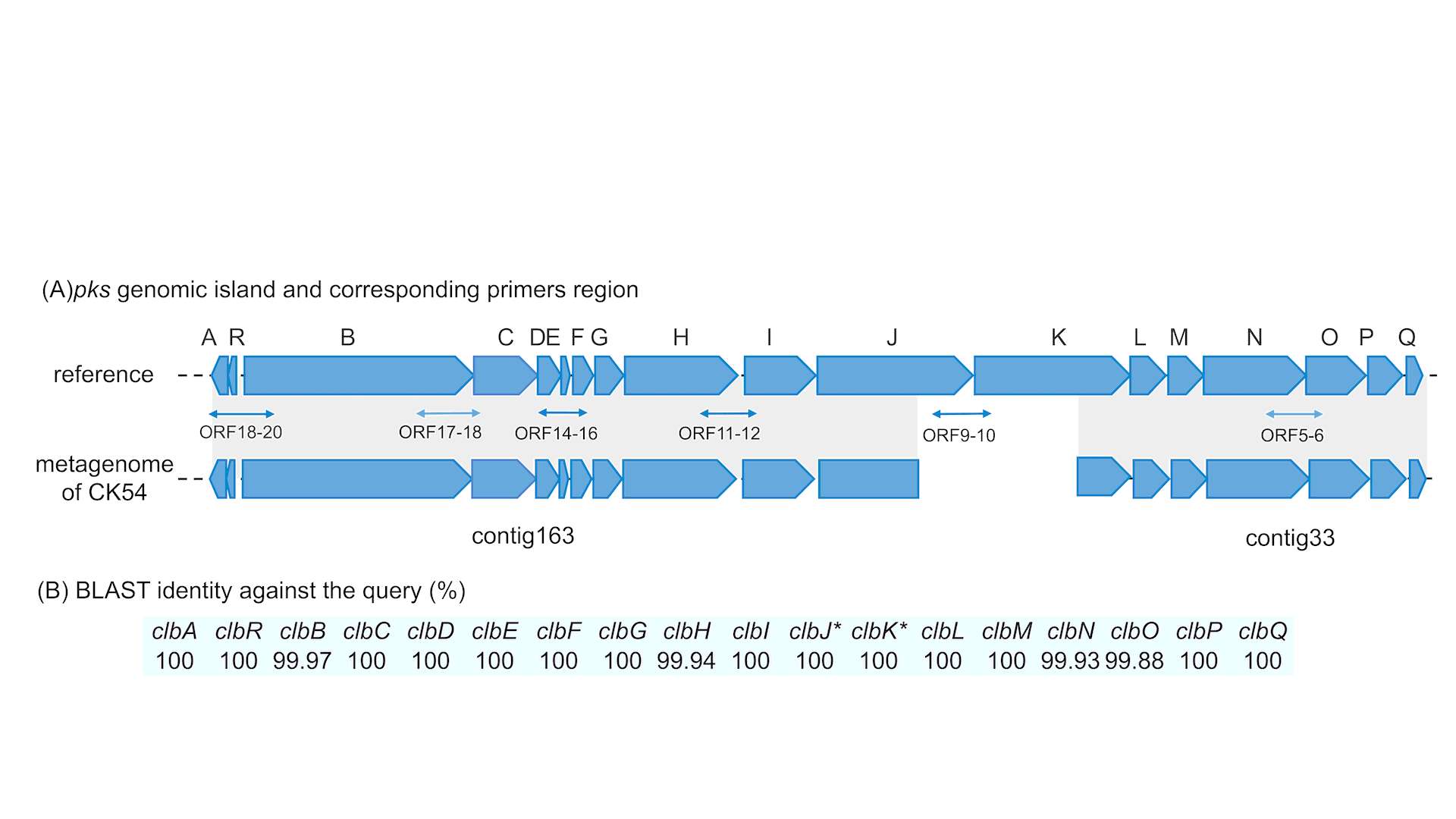
Detection of colipolyketide synthase (pks) genomic islands in cultured bacteria isolated from bile acid
Library construction for an Illumina MiSeq instrument and subsequent de novo assembly of raw reads by the CLC Genomics Workbench (v 8.0) software package (Qiagen, Valencia, CA) were performed as previously described[19]. Open reading frame (ORF) prediction and annotation were performed using the DDBJ Fast Annotation and Submission Tool (DFAST) with the default settings[20]. Colibactin genomic islands were detected by BLASTP analysis against NCBI reference sequences WP_001217110.1, WP_000357141.1, WP_001518711.1, WP_001297908.1, WP_000982270.1, WP_001297917.1, WP_000337350.1, WP_000159201.1, WP_001304254.1, WP_000829570.1, WP_001468003.1, WP_000222467.1, WP_001297937.1, WP_000217768.1, WP_001327259.1, WP_001029878.1, WP_002430641.1 and WP_000065646.1. PCR for the corroboration of the existence of pks-islands was performed as previously described[21]. The region of primers for the pks-island is shown in Supplementary Figure 1.
Statistical analysis
Permutational multivariate analysis of variance (PERMANOVA) based on the UniFrac distances was used to evaluate interindividual variability among groups by using the ‘adonis’ function in the vegan R package (ver. 3.3.0), and p-values of < 0.05 were considered statistically significant. Linear discriminant analysis (LDA) effect size (LEfSe) was performed with default parameters to identify microbial taxa that were differentially abundant among groups[22].
Data deposition
DNA sequences corresponding to the 16S rRNA gene and metagenome data have been deposited in DDBJ under accession numbers DRA011518 and DRA011520, respectively.
{kind=link}
{kind=link}
{kind=link}
{kind=link}