In this study, citrate-phosphate-dextrose adenine anticoagulated WB refrigerated for 24 hours showed better AA and ADP-induced platelet aggregation and metabolism than WB stored at RT. The ROTEM results, platelet counts, and fibrinogen levels were stable for cold-stored WB and were comparable to the changes observed in WB stored at RT.
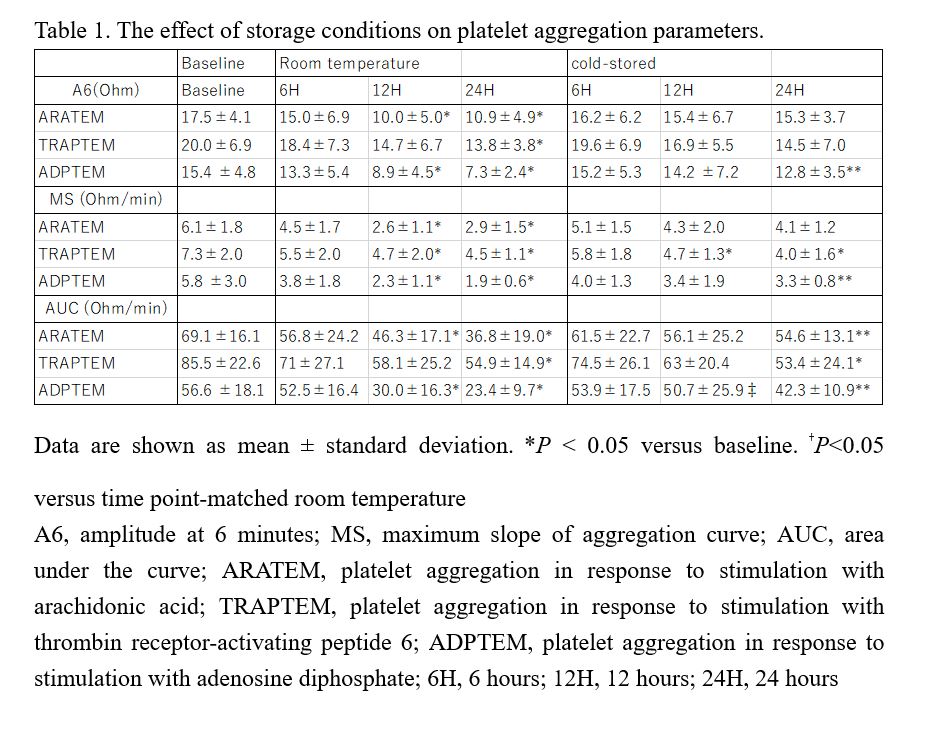
The markedly reduced ability of platelets stored at RT to aggregate upon stimulation with AA and ADP may be attributed to the progressive deterioration of the energy generating mechanism.15 The transition of platelets from a quiescent to activated state increases ATP demand.
In contrast, platelets stored at 4°C exhibit better aggregation when stimulated by AA and ADP than those stored at RT after 12 hours of storage which is consistent with a previous report,9,10 and is possibly caused by cold-induced platelet activation triggered by a rise in intracellular calcium. Calcium influx activates specific signaling pathways and facilitates release of granule contents, amplifying platelet activation during cold storage.16 Active glycoprotein IIb/IIIa receptors play a central role in the cross-linking of fibrinogen or Von Willebrand factor among receptors to mediate platelet aggregation.17 A similar decline in aggregation induced by TRAP at both storage temperatures may be caused by a reduction in the number of high-affinity thrombin-binding sites, inducing platelet secretion and aggregation.18
Glucose consumption was slower for cold-stored WB than that for the RT counterpart, wihch concurs with the lower glycolytic metabolism of cold-stored WB.9 Lactate levels increased gradually in the cold-stored WB, whereas significantly elevated lactate levels were observed in the RT-stored WB after 6 hours. The glycolytic pathway is accelerated during ex-vivo storage of WB under hypoxic conditions, leading to consumption of glucose and consequent accumulation of lactate and free hydrogen ions, which are buffered by bicarbonate to yield carbon dioxide and water.19
The metabolic assay data of this study showed signs of storage lesions at as early as 6 hours of storage at RT, which may have caused the changes in platelet aggregation. When the supply and demand of energy are imbalanced, platelets rapidly lose their capacity to respond to aggregation- and secretion-inducing agents.20 Stable pH and glucose levels preserve platelet viability against activating stimuli caused by storage.21–23 Thus, the nearly constant pH and glucose levels of platelets in cold-stored WB indicated that the quality of platelets maintained by refrigeration is better.
WB aggregometry is particularly dependent on platelet count even within the normal range.24 Although platelet counts in cold-stored and RT-stored WB are nearly similar, platelets stored at RT lose their ability to aggregate to chemical stimuli. Thus, the activation state attained by circulating platelets may differ from that attained during storage, which is related to aging and time-dependent structural and functional changes indicative of platelet storage lesions.
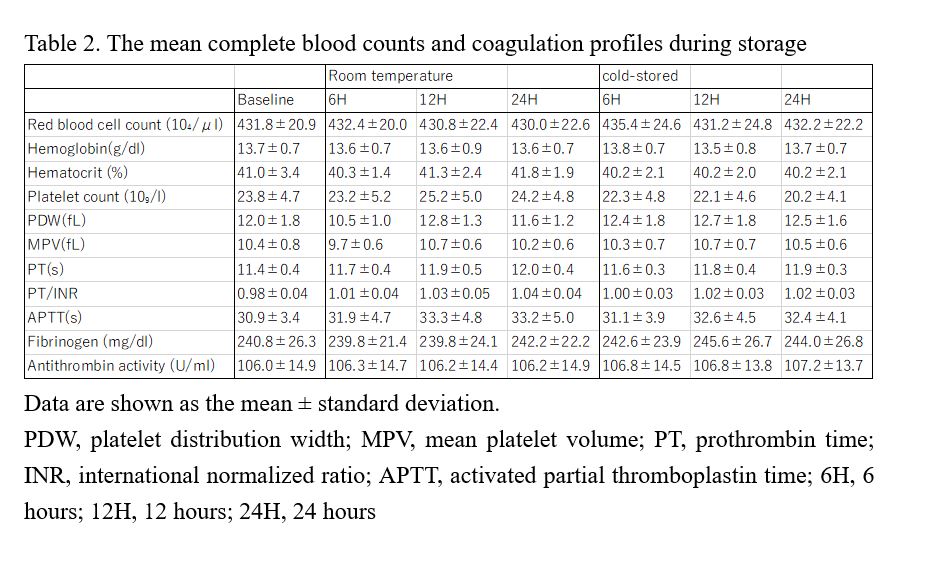
Mean platelet volume and platelet distribution width remained unchanged in both RT and cold-stored samples, suggesting no significant changes in the size of single platelets and platelet size distribution, a finding in contrast with those of previous studies,12,25 where refrigeration induced changes in platelet shape from disks to spheres in 24 hours. However, these studies assessed platelet concentrates (PC) prepared from WB or buffy coats. Thus, the difference between WB assays and diluted PCs must be considered, because WB has significant pH-buffering capacity,26 which affects platelet morphology and in-vivo recovery.
Our data showed that PT, APTT, fibrinogen level, and antithrombin activity in WB stored at both temperatures for ANH were maintained within normal reference limits over the 24-hour storage period. This observation is consistent with that of a previous study11 where most coagulation proteins stored in WB were not significantly depleted and were maintained above the lower reference limit for at least 24 hours, which is the permissible storage time before component preparation in some countries, including the United Kingdom and Canada.
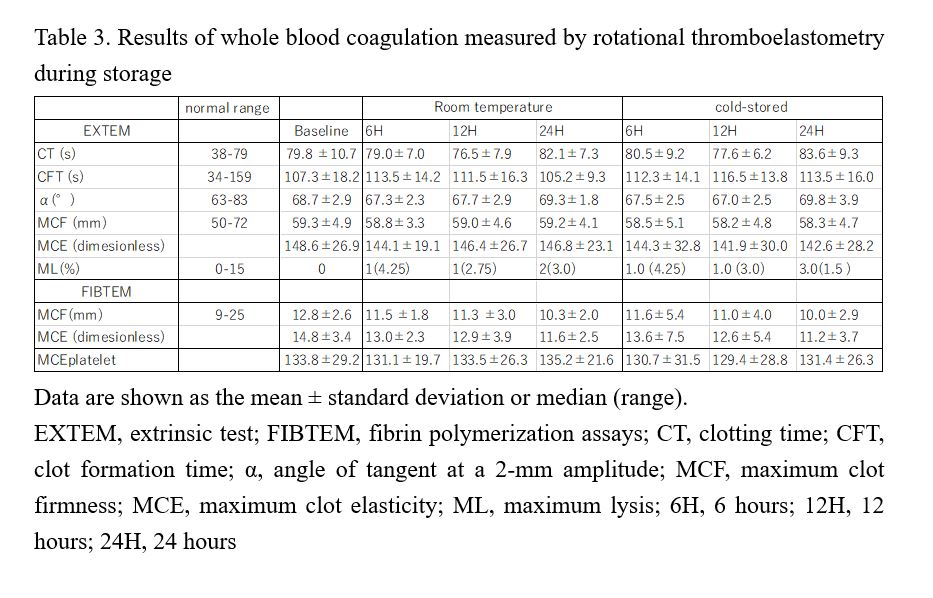
In our study, the average EXTEM CTs of RT and cold-stored WB samples over time were slightly higher than the reference range; however, the differences would not be clinically significant as the ROTEM-guided transfusion algorithm recommends the administration of coagulation factors when the EXTEM CT exceeds 100 s. The platelet component of clot strength, measured by clot elasticity in both stored samples remained constant, showing that the clotting ability of cold-stored platelets was comparable to that of platelets stored at RT, despite better metabolic indices and aggregation response. The discrepancy between progressively reduced platelet aggregation response and constant platelet components as a result of ROTEM could be attributed to the sensitivity of viscoelastic tests to platelet function. Clot firmness is directly proportional to platelet counts and is associated with platelet function depending on the transmission of platelet contractile force to fibrin,27 which is the final step in platelet aggregation, mostly mediated by glycoprotein IIb/IIIa receptors. However, the thrombin formed extensively by the activators of viscoelastic tests interacts with protease-activated receptors and bypasses other pathways. Therefore, ROTEM is not sensitive to drugs acting on the thromboxane pathway or the P2Y12 ADP-dependent receptors and does not reflect impair platelet function.28
This study had some limitations. First, it was based solely on in-vitro experiments conducted under static conditions, which could result in different platelet functions and kinetics when administered in vivo. Thus, our observations should be complemented with clinical trials to compare the in-vivo properties of RT and cold-stored WB for hemostasis during surgeries. Second, cold storage induces many changes in platelets not corresponding with aging or storage lesions of platelets stored at RT. These changes can be influenced by several factors such as the levels of surface-receptor modifications, platelet-activation markers, and thrombotic microparticles, that were not measured herein.
This study demonstrated that RT-stored WB showed the development of stored lesions after 6 hours and lost platelet aggregation response after 12 hours of initial collection compared with cold-stored WB, as determined by blood gas levels, coagulation profiles, and aggregation responses. These data suggest that cold-stored WB has better metabolic and functional competence than RT-stored WB, although a more comprehensive analysis of coagulation profiles and hemostatic effects in clinical settings are required to confirm our findings.
{kind=link}
{kind=link}
{kind=link}