Liver resection is a curative surgery for many benign and malignant disorders, with the most common indications are hepatocellular carcinoma and colorectal liver metastasis. Liver resection was historically associated with very high morbidity and mortality, which has now decreased significantly due to improved surgical and anaesthetic techniques and improved perioperative and critical care. Complications and hence morbidity rates though decreased but remain very high and range between 20-40%. [14-58]. There are also wide regional variations in indications of liver resections. In Asian countries, the most common indication is hepatocellular carcinoma [59] while in European countries most common indication is colorectal metastasis, which can also be the reason for variable mortality following liver resection.
Our aim in conducting this systematic review and prevalence meta-analysis to study weighted post-operative morbidity rates after liver resections. We also aimed to look at the heterogeneity of the analysis and publication bias. We also did metaregression analysis for various factors affecting mortality like Major hepatectomy, blood loss, age, open resections, a cirrhotic background of the liver, and etiologies for resections like hepatocellular carcinoma and colorectal metastasis in a study published in the last 5 year to look for recent trends.
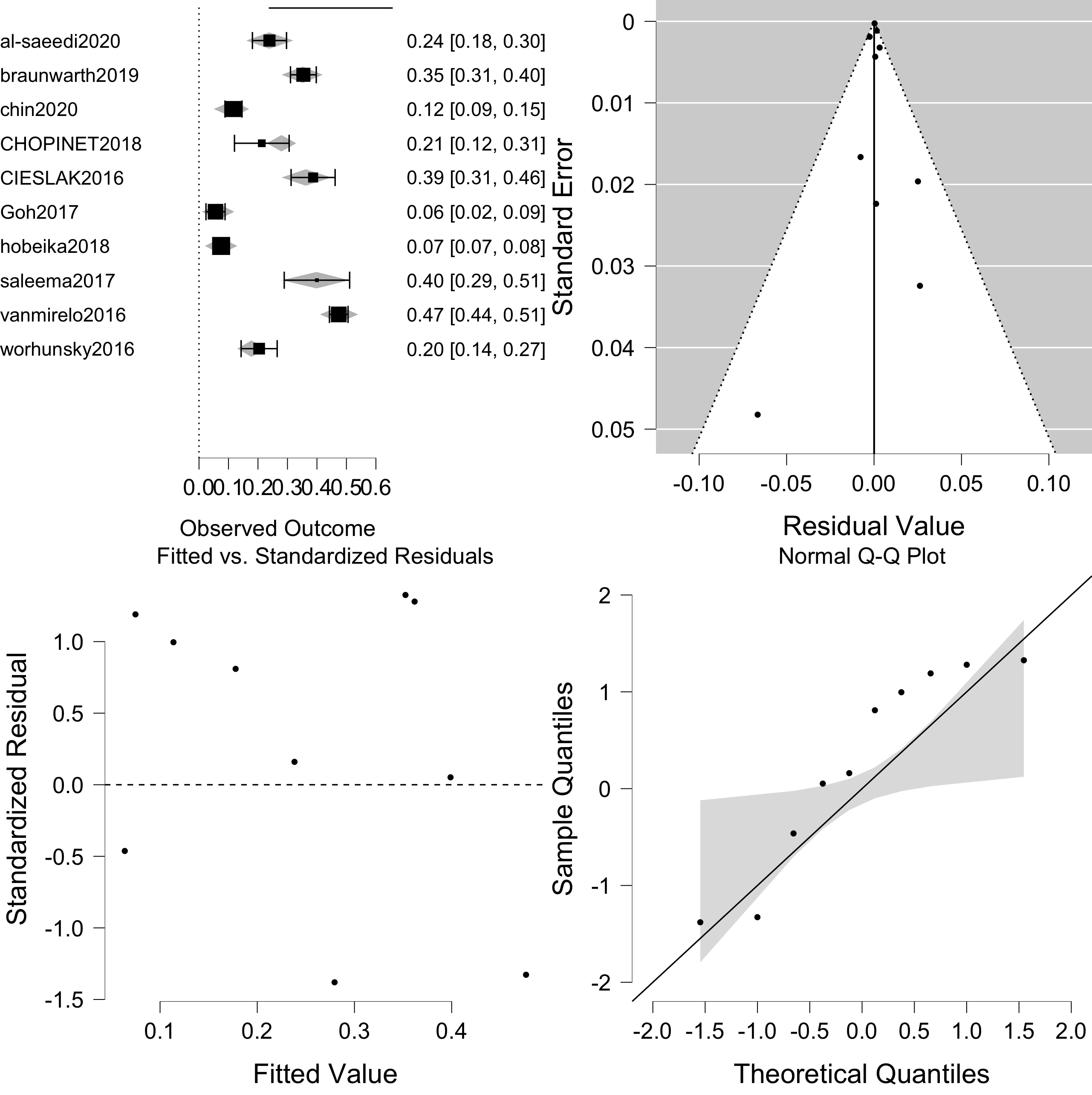
As shown in figure 3, Weighted post-operative morbidity was 30.2% ( 95 % C.I. 24.8-35.7%). However, the heterogeneity of the analysis was significantly high. On univariate metaregression, only major hepatectomy was significantly associated with heterogeneity and hence morbidity but residual heterogeneity was still significantly high. After multiple factor metaregression entering all above factors as covariates, residual heterogeneity was moderate and not significant with p=0.189 and I2 39.99%. Elimination of residual heterogeneity after metaregression suggested that the above factors were mainly responsible for variable outcomes across the centres.
On multiple factor metaregression major hepatectomy, age, open surgery, cirrhotic background, blood loss, and colorectal liver metastasis were associated with heterogeneity and morbidity. As shown in table 2 major hepatectomy, open surgery, and cirrhotic background were having positive metaregression coefficients and z value suggesting a positive relationship which means higher the number of major hepatectomies, open surgery and surgery on cirrhotic liver higher the chance of positive effect size and hence higher morbidities. Colorectal liver metastasis was having a negative metaregression coefficient and z value suggesting higher the number of liver resections for colorectal liver metastasis lower the effect size and hence morbidity.
Blood loss and age were having negative metaregression coefficients and z value suggestive of negative correlation or inverse relationship between effect size or morbidity and them. This might be due to patients with older age or more blood loss have higher post-operative mortality even before complications happen. Their positive correlation with 90 days postoperative mortality has been reported by us in a similar meta-analysis with metaregression analysis under review for publication and available as preprint online. [60].
Limitations of the meta-analysis were a large number of studies had to be excluded due to lack of complication data [61]. Also, we could not take into account centre volume and surgeon’s experience. Another limitation was only 10 studies mentioned all the moderators however, the number of studies was adequate to conduct metaregression analysis.
However, to our knowledge, this is the first meta-analysis that evaluated weighted post-operative morbidity rates and evaluated various factors responsible for heterogeneity and lack of significant residual heterogeneity after metaregression proved their effects on variable morbidity rates across the centres.
In conclusion, postoperative morbidity rates may vary according to centres based on various factors mentioned above. Major hepatectomy, open surgery, the cirrhotic background may be associated with higher morbidities and liver resection for colorectal liver metastasis may be associated with lower postoperative morbidity compared with other etiologies like hepatocellular carcinoma.
{kind=link}