To our knowledge, this study provides some of the most mature RWD about treatment outcomes from a single institute and serves as a report on how results from RCTs translate to patients in routine clinical practice.
Although the OS rate of PC patients is one of the worst in any disease, our data clearly show the benefit of active treatment. As seen in Fig. 2a, the treated group had a significantly longer OS than the untreated group. Active treatment results in several additional months of life. Extending the life expectancy from 2.8 months to 10.4 months (Fig. 2a) is significant, and it is important to discuss this possibility with every patient diagnosed with PAC. Furthermore, our analysis showed a clear benefit of surgery in patients with resectable disease and, to some extent, those with locally advanced disease. Patients who received neoadjuvant or adjuvant chemotherapy achieved a median OS of 31.2 months compared to 8.7 months for patients receiving 1L chemotherapy and 2.7 months for untreated patients (Fig. 2b). While locally advanced disease is usually inoperable, a few of our patients with locally advanced disease underwent surgery. Our study also clearly showed the generally more favourable median OS of patients diagnosed with locally advanced disease compared with the OS of those diagnosed with metastatic disease (9.2 vs. 4.9 months) (Fig. 2c). This indicates the need for better diagnostic tools, such as biomarkers, and better imaging technology, to increase the number of patients who are diagnosed at an earlier stage of disease, as other studies have also shown (34–38); novel therapies are also needed.
Increasing the treatment duration and number of treatment lines administered resulted in a significant increase in OS from 6.3 months with one line of treatment up to 19.1 months with 3 or more lines of treatment (p < 0.002) (Fig. 3b). This finding is subject to survival bias, with healthier patients living longer and therefore receiving more treatment. It is thus not necessarily the treatment that is prolonging their lives. Further research on the subject is needed before conclusions can be drawn. However, these results provide evidence of the benefit of treating younger patients with lower ECOG scores more aggressively for longer periods of time.
Even though our data largely show relatively short survival times after diagnosis, there were some individual cases that stood out. A few patients treated early during our study period were still alive after 5 years and showed no signs of disease, with one patient showing complete remission of disease (confirmed via radiological examination) after a single cycle of gem monotherapy (PAD was positive for PAC). While this outcome is rare and further research is needed, these cases may serve as a source of hope for researchers, clinicians and patients because they show that remission can occur.
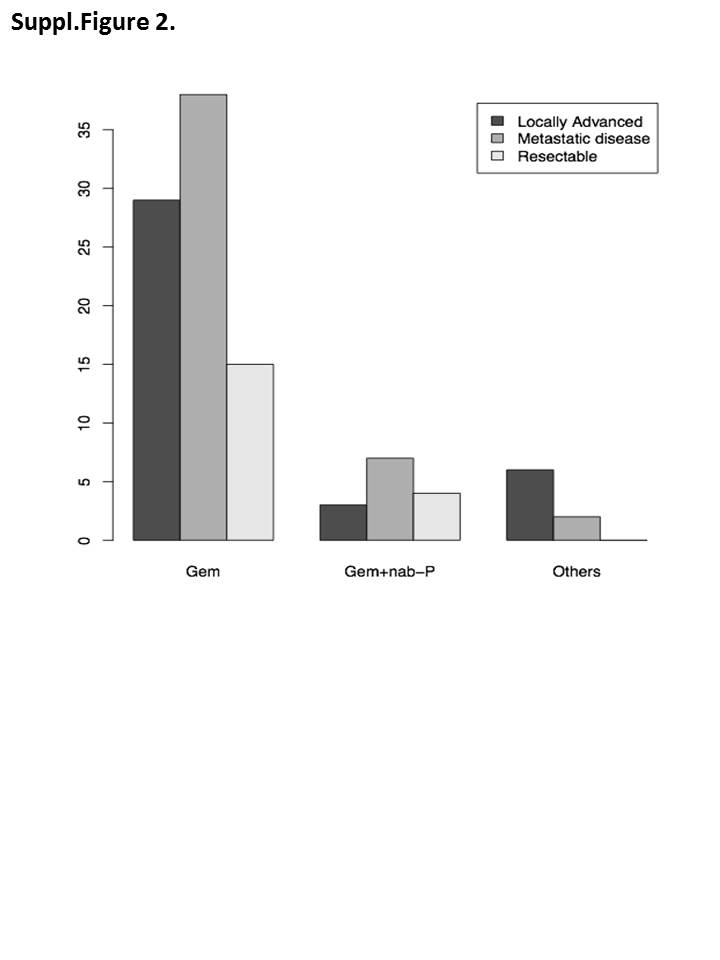
Because the combination of gem + nab-P was approved for PAC rather late during our follow-up period, the number of our patients who received this combination was low. Seven patients received gem + nab-P as a 1L treatment, while 63 patients received gem monotherapy, and 8 patients received another treatment. This limited our analysis of the efficacy and safety of this combination compared to the efficacy and safety of gem monotherapy.
To better assess the efficacy of gem + nab-P combination treatment, we analysed the OS of patients who received gem + nab-P at any time during their treatment schedule (among all treated patients and in the subgroup of patients with metastatic disease). The results were fairly conclusive; in all patients using gem + nab-P, the median OS was 18.3 months, which was longer than the 7.3 months in patients receiving other types of treatment, including gem monotherapy (p < 0.008). This analysis included all patients (except patients who had undergone surgical resection of the tumour) (Fig. 4a). In the subgroup of patients with metastatic disease, the results were also promising, with those who received gem + nab-P obtaining a median OS of 11.2 months, while those who received other treatments obtaining a median OS of 6.3 months; however, this difference lacked statistical significance (p < 0.112) (Fig. 4b).
Due to its poor toxicity profile and the older age and poor performance status of our population, no patients in our study received FOLFIRINOX. Our analysis shows that there were significant toxicities and safety concerns associated with the administered treatments. A total of 10 (7 with recorded AEs and 3 without known cause) patients died within 30 days of chemotherapy administration. The most commonly observed AEs were grades 2–4 bone marrow toxicities, nausea, diarrhoea and infections. The frequency of AEs was high, with almost every patient experiencing an AE and many patients experiencing more than one. Grades 2–5 AEs occurred most frequently in the metastatic subgroup (134 out of 281), closely followed by the locally advanced subgroup (86 patients).
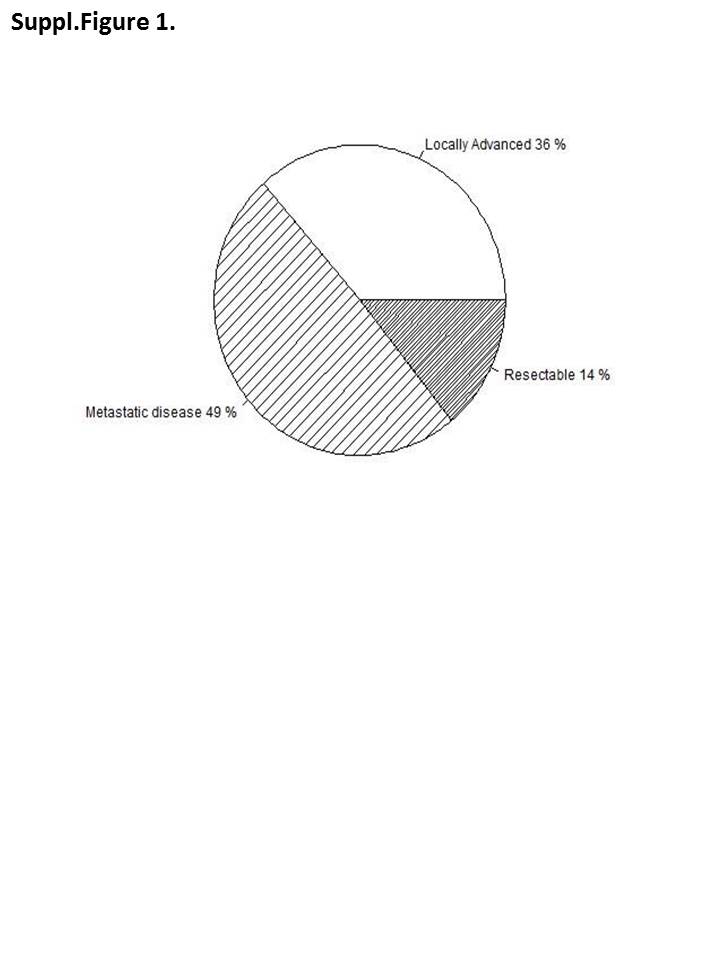
Due to key similarities in patient characteristics and geographical location, we used the results from the 2019 study by Bloomberg et al. (29) as a reference and compared the results to our own. We also considered the results from the landmark MPACT study by Von Hoff et al. from 2013 (12) when analysing our own results. However, due to significant differences between the inclusion/exclusion criteria and the manner in which our study was completed, a direct comparison of results between the MPACT study and our retrospective report is not possible. The present study and the study by Blomstrand et al. included all diagnosed cases of PC, with 50.7% of our patients having locally advanced or resectable disease, while the MPACT study only included patients with confirmed metastatic disease who were relatively young and in good condition.
Bloomberg et al. performed analyses to compare their results with those of the MPACT trial. Their study showed a longer estimated median OS for patients with metastatic disease than the median OS observed in the MPACT trial (9.4 vs 8.9 months), while our cohort had an estimated median OS of only 4.9 months. However, our patients in the metastatic subgroup were significantly older and in worse condition than those included in the MPACT trial or the study by Blomstrand et al., with 36 out of 73 patients with metastatic disease older than 70 and 64 patients with an ECOG score of 2 or 3. In the MPACT study, 58% of the patients were younger than 65 years and had a Karnofsky score > 60, which is equivalent to an ECOG score of 0–2. The MPACT study included only patients with metastatic disease, whereas we included all diagnosed patients. (12, 13)
Our study showed a mildly improved survival for patients in all three subgroups who received 1L chemotherapy (regardless of disease stage) compared with the MPACT trial. Our patients receiving gem monotherapy had a median OS of 7.7 months (vs MPACT 6.7 months), those receiving gem + nab-P had a median OS of 10.5 months (vs MPACT 8.5 months), and those receiving other therapies had a median OS of 18.5 months (p < 0.171). Our analysis was conducted with all patients receiving 1L chemotherapy (not including patients who underwent surgical resection) due to the small patient population. Notably, however, we obtained very similar results in terms of OS when compared with the study by Blomstrand et al.; their patients had a median OS of 10.9 months compared to the OS of 10.5 months in our gem + nab-P subgroup.
The results of the study by De Vita et al (39) and a meta-analysis of 50 studies presented at an international conference suggest that with careful and appropriate patient selection, a median OS of longer than 12 months can be attained with 1L gem + nab-P (40).
The patients in the present study experienced AEs more frequently and with higher grades than those in the study by Blomstrand et al., the MPACT study and previous studies on the subject (41, 42). The most common side effects in the aforementioned studies were bone marrow toxicities. Since no data on dosage have been published, we cannot with confidence determine the cause of this discrepancy. Both of the studies used for comparison collected data from 1L treatment only, while the present study included all treatment lines, with a large proportion of patients receiving 2 or more lines (36%) and 15 patients receiving 3 or more lines. This increased exposure to therapy regimens and longer follow-up time coupled with advanced age and high ECOG scores might contribute to the higher numbers of AEs observed.
While Blomstrand et al. published RWD, there are key differences in the design of our study. The primary difference is that they examined the efficacy of gem + nab-P combination therapy in a real-world population and compared their findings with the established MPACT study. Our study is mainly a retrospective report of the outcomes in all treated PAC patients in a hospital in central Finland during an approximately six-year period. However, our study provides important and mature data with substantial value to clinicians. The present study included every patient diagnosed with PAC regardless of insurance status, comorbidities, age, sex, ethnic subgroup, or socioeconomic status and therefore provides a very close approximation to the outcomes of treatment with many of the accepted therapies today in patients in Finland diagnosed with PAC.
The present study involved a heterogeneous patient group, which made analysis and interpretation of the results difficult and, to some extent, impossible. The heterogeneity and lack of standardization in 1L treatment regimens was the most disruptive factor and is also the largest limitation of our study. Due to these limitations, direct evaluation of efficacy between individual treatment regimens was not feasible.
We believe that the treatment decisions made during our study period were influenced by an array of factors, including age and ECOG score at baseline, which could partly explain why a relatively small number (only 77 out of 148 patients) received chemotherapy as a 1L treatment and only 7 patients initially received gem + nab-P combination therapy. Furthermore, the fact that change has been slow in the field of PAC treatment, with no new regimens introduced between 1997 and 2011/2013 that were improvements compared with gem monotherapy, together with the many years of clinical experience with the use of gem monotherapy, can provide an explanation for the low number of patients receiving 1L combination therapy.
In our study, AEs frequently occurred during chemotherapy administration. The frequency was higher than that reported in the literature, mainly because our patients were older and had worse performance status scores. Seven patients died during treatment. Another three patients died without clear signs of disease progression; these deaths were registered as treatment-related deaths, but none of these patients died after the first chemotherapy cycle. This means that the initial chemotherapy was tolerated, but as treatment was continued, the level of toxicity became too high in some patients. Notably, among the patients who died during treatment, one patient who died had resectable disease, was 65 years old, and had an ECOG score of 2; thus, this patient should have had a more favourable prognosis and should have been treated actively. Another patient who died from AEs had metastatic disease, was older than 70 years and had an ECOG score of 2. Similarly, 5 other deaths occurred in patients with locally advanced disease, who were over 70 years old and, with the exception of 1 patient with an ECOG score of 1, had ECOG scores of 2. Overall, in our study population, 106 patients (72%) had an ECOG score of 2 and a median age of 70.7 years, and 50% of the study patients were older than 70 years. Therefore, if active treatment had been denied to patients older than 70 years or who had ECOG scores of 2 or more, then most of our patients would not have had the chance to obtain the clear benefit they received from active treatment with chemotherapy. However, we think that performing more active follow-up during treatment and allowing temporary or permanent discontinuation of therapy might affect the occurrence in side effects and decrease the number of treatment-related deaths. In addition, based on our data, those patients who can tolerate it should continue therapy.
These findings strongly suggest the need for more tolerable therapies and more research to further establish patient selection criteria for every treatment regimen; treatments are especially needed for patients with ECOG scores of 2 and those with metastatic disease who are in good condition. Further research is also needed on protocols and patient selection criteria for the continuation of treatment beyond the 1L. This coupled with definitive protocols based on evidence regarding when and which patients should receive palliative care instead of continuing with active therapy could also save resources. Furthermore, this study clarifies the need for RWD to supplement RCTs. Analysis of RWD could reduce severe side effects and deaths caused by overtreatment, providing a reference for individual physicians when determining the best treatment for patients with PC.
In the last few years, the efficacy of 1L FOLFIRINOX or gem + nab-P vs gem monotherapy for metastatic PAC has been widely investigated. Since no three-arm RCTs measuring efficacy have been conducted, real-world observations are important to inform decision making. Many studies have hinted that the OS achieved with treatment with FOLFIRINOX is slightly superior to that achieved with gem + nab-P (14.1 compared to 10.5 months according to Wang et al 2019 or 17.1 compared to 11.5 months according to Sasaki et al 2019) (28, 43). However, the same studies also concluded that FOLFIRINOX should be reserved for a very small portion of the patient population due to its toxicity profile. Aroldi F et al. proposed the following treatment algorithm for metastatic PAC: patients with a performance status score of 0–1, who are younger than 65 years and who have no comorbidities can receive FOLFIRINOX as a 1L treatment; patients with an ECOG score of 0–1 who are older than 65 years should receive gem + nab-P as a 1L therapy; and patients with an ECOG score > 1, who have serious comorbidities and are older than 65 years should receive gem monotherapy as a 1L treatment (18). After disease progression, Aroldi F et al. proposed that the 2L treatment should depend on the 1L treatment. Patients who received 1L FOLFIRINOX should receive gem + nab-P or gem monotherapy, those who received 1L gem + nab-P should receive either platinum-based therapy (Xelox, Gemox or OFF), irinotecan-based therapy (FOLFIRI, Nal-Iri, Nal-Iri + 5-FU-leucovorin) or fluoropyrimidine, and patients who received 1L gem monotherapy should receive irinotecan monotherapy or fluoropyrimidine after consideration of the condition of the patient (18). Most studies recommend 2L therapy for patients who are able to tolerate it, with a few studies describing prognostic factors for receiving and benefiting from 2L therapy (23, 25, 26). For example, Vienot et al. (26) presented a prognostic model to predict which patients would benefit the most from 2L therapy. Their study found that age, smoking status, liver metastases, ECOG performance status score, jaundice, duration of 1L treatment, type of 1L regimen and pain were prognostic factors. Pokataev et al. (23) provided another prognostic model to predict which patients would benefit the most from 2L chemotherapy. In their study, poor Karnofsky performance status (less than 70%) and a neutrophil-to-lymphocyte ratio > 5 (NLR) were independent negative prognostic factors for a benefit of 2L therapy. Tsang et al. (25) performed a multivariate analysis and found that a better ECOG score, locally advanced disease and 1L treatment with FOLFIRINOX were the best prognostic factors for receiving a benefit from 2L therapy. All of these proposed prognostic factors need to be validated in prospective studies. However, these studies provide a preliminary list of factors clinicians should pay attention to when deciding whether to administer 2L treatment to patients.
PAC is unfortunately often diagnosed in a late stage, thus substantially narrowing the treatment options and leading to a poor outcome. There is an urgent need for new techniques and biomarkers to facilitate the diagnosis of PAC in an earlier stage and to facilitate therapeutic decision making and the determination of follow-up strategies. Liquid biopsies (LBs) are a promising non-invasive approach to the generation of personalized cancer treatment strategies. Improvement in LB techniques is urgently needed as is the standardization of LB protocols. However, these techniques are becoming widely recognized as fundamental tools in clinical practice, as highlighted in the meta-analysis conducted by Luchini et al. (44).
Unfortunately, long-term remission of PAC remains rare, even with the current standard treatments, namely, chemotherapy and surgery, and personalized medicine. This indicates the urgent need for new therapeutic and diagnostic strategies. To this end, the POLO RCT indicated that therapy with olaparib significantly delayed the progression of metastatic PAC with a BRCA germline mutation (45). While immunotherapy (IO) has been increasingly important in many other cancers, it has not been shown to be effective in PAC. Efforts have been made to broaden the impact of IO in PAC, focusing on the stimulation of the anti-tumour T-cell response and the enhancement of tumour sensitivity to chemotherapy (46). Currently, however, it remains unclear whether concurrent chemotherapy and IO is a viable therapeutic approach. Preclinical studies have shown the potential success of this combination, but practical clinical evidence has not yet been obtained.


{kind=link}
{kind=link}