Serum CA125 levels and the six monosaccharide concentrations in hydrolyzed serum glycans were different among the control, EC, and uterine fibroid groups.
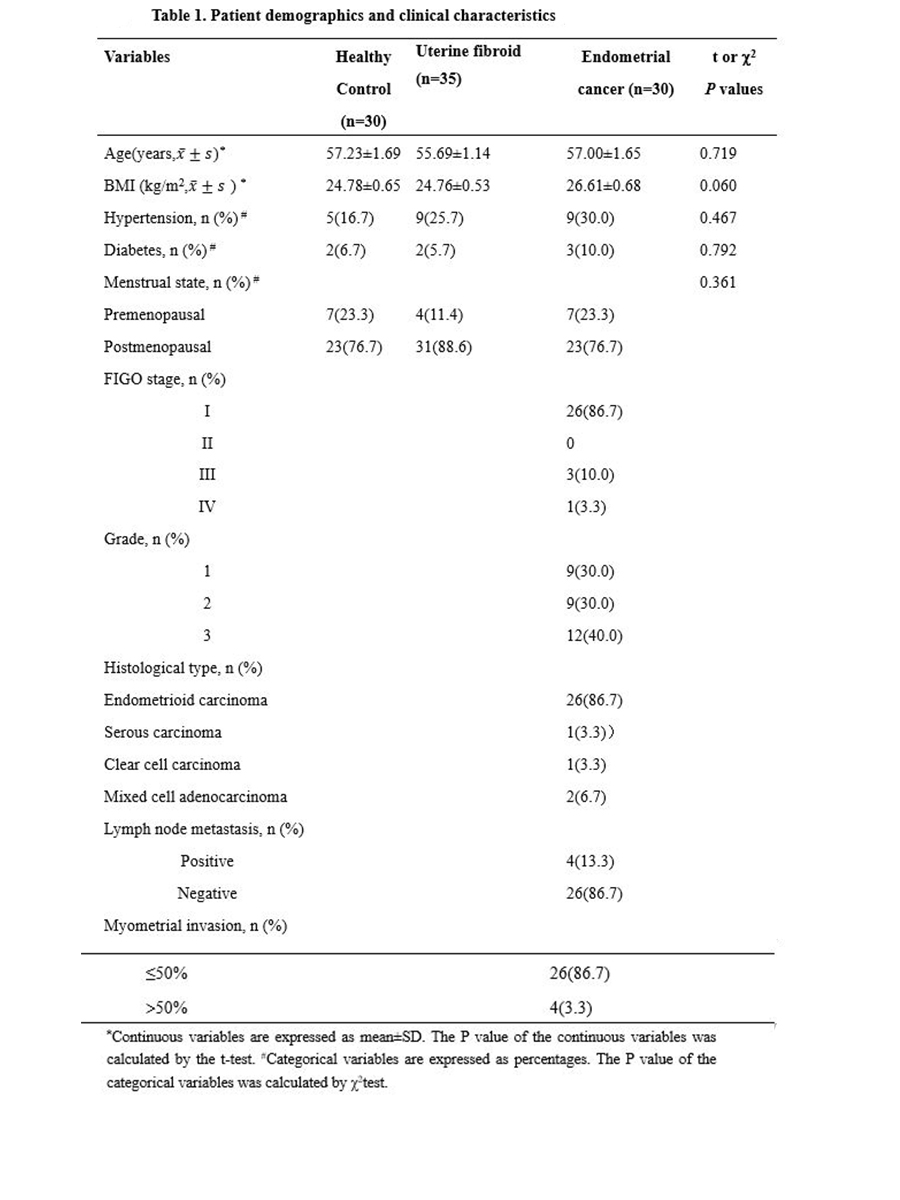
The demographic and clinical characteristics for patients and healthy individuals are summarized in (Table 1). The average ages were 57.00 ± 1.65 years for EC patients, 55.69 ± 1.14 years for patients suffering uterine fibroid, and 57.23 ± 1.69 years for the healthy control group (P = 0.719). There were also no statistically significant differences in BMI (P = 0.060), menopausal status (P = 0.361), hypertension (P = 0.467), and diabetes (P = 0.792).
Serum CA125 levels were shown in (Fig. 1a) for the three groups. The increased median CA125 levels were observed in the uterine fibroid group compared to that in the EC, and the control groups. Uterine fibroid group had significantly increased serum CA125 levels compared to the control group (p < 0.0001) as well as to the EC group (p < 0.01), which was consistent with our previous finding that CA125 is associated with fibrosis-associated diseases more than with cancers[31].
The concentrations of six monosaccharides, including Fuc, Gal, GalN, Glc, GlcN, and Man, in hydrolyzed serum samples of all three groups obtained by our optimized method[32] were summarized in (Fig. 1b). Median Gal and Glc concentrations were significantly increased (P < 0.05), whereas Fuc concentration was significantly decreased (P < 0.05) in hydrolyzed serum glycans of the EC group compared to the control groups. Unexpectedly, all six monosaccharide concentrations were significantly different (P < 0.05) between the EC and uterine fibroid groups. Remarkably, Man, GlcN, and Gal concentrations were only significantly decreased in the uterine fibroid group compared to the control group. Moreover, Glc concentration was significantly increased (P < 0.05) in the EC group but significantly decreased (P < 0.05) in the uterine fibroid group compared to the control group.
Monosaccharide concentrations in hydrolyzed serum glycans were potential early diagnostic biomarkers for EC.
Early diagnosis will be critical in preventing EC-related death. We next tested if the monosaccharide concentration changed at the early stages of EC development. Figure 2 showed significantly changes in Fuc (P = 0.001), GalN (P = 0.04), and Glc (P = 0.04) concentrations were present in stage I/II. No significant changes in six monosaccharide concentrations were observed between the EC patients at stage I/Ⅱ and stage Ⅲ/IV. Thus, the monosaccharide concentration changes occurred in the stage I/Ⅱ of the EC development, which made them suitable for the early EC diagnosis.
Monosaccharide composite of hydrolyzed serum glycans was a better biomarker than CA125 for the EC diagnosis
We next investigated the diagnostic properties of CA125, six monosaccharides from hydrolyzed serum glycans, and the monosaccharide composite as EC biomarkers by performing the receiving operator curve (ROC) analysis (Fig. 3). Since all six monosaccharide concentrations were obtained and quantified in the same chromatogram of a HPLC analysis, we used logistic regression analysis to test the monosaccharide composite as biomarker for EC diagnosis. The following logistic regression model for monosaccharide composite was established:
-12.131-13.909Man-1.666GlcN + 41.358GalN + 1.873Glc + 20.977Gal − 26.359Fuc. The detailed AUC, 95% confidence interval (CI), sensitivity, specificity, accuracy, positive predicting value (PPV), negative predicting value (NPV) and P values for CA125, each monosaccharide, and the logistic regression model were summarized in Table 2.
Among the monosaccharides, the AUC value for Fuc was the highest (0.75, 95% confidence interval, 0.63–0.87, P < 0.001). Using 0.32 mmol/L as the cutoff value, the sensitivity and specificity for Fuc as a biomarker for EC diagnosis were 56.7% and 86.7%, respectively (Fig. 3), which were better than CA125 as a biomarker for EC diagnosis. The AUC for monosaccharide composite as a biomarker for EC diagnosis was further increased to 0.96. The area under curve (AUC), 95% confidence interval, sensitivity, specificity, and accuracy were 0.96, 0.92-1.00, 86.7%, 93.3%, and 90.0% for monosaccharide composite biomarker and 0.58, 0.43–0.73, 40.0%, 83.3%, and 61.7% for CA125, respectively (Table 2). Therefore, the monosaccharide composite had the advantage over any single monosaccharide or CA125 as a circulating biomarker for EC diagnosis.
When the cutoff value was set at 0.396 for the logistic regression model, the novel monosaccharide composite biomarker detected 28while CA125 only detected 5 out of 30 EC patients (Fig. 4). Thus, monosaccharide composite was an excellent biomarker for EC diagnosis.
{kind=link}