A broad range of non-neoplastic and non-infectious DPLD existed under the less specific umbrella term of ILD. This large group of diseases included those with histopathological findings identical to IIPs but with known etiology, commonly connective tissue diseases and respiratory exposures, and those with defined clinical, radiological, and pathological definitions including lymphangioleiomyomatosis, sarcoidosis, pulmonary Langerhans cell histiocytosis, and eosinophilic pneumonia. Some neoplastic or infectious processes masquerading as suspected ILD by diffuse abnormalities were also commonly encountered. So, the pathological diagnosis only from pulmonary parenchyma wasn’t enough in some conditions. Microbiological and cytological information might also be needed in these cases. The progress of transbronchial techniques ensured all these procedure to be performed at the same examination. BALF was not always required in the assessment of the IIPs but to exclude infection or tumor [2,3]. TBLB was used to excluding infection and tumors and not for diagnosis of IIPs because traditional forceps yielded small biopsy samples with significant crush artifacts which were only sufficient for 20–30% and occasionally misrepresented the overall diseases [6]. Many studies indicated that the mean length and area of the specimens from lung parenchymal tissues by TBLC were substantially larger than TBLB, and the specimens didn’t have crush artifacts [6,10,12,13,14]. Samples obtained through TBLC contained peripheral structures of the secondary pulmonary lobules [8]. There was a significant difference between TBLC and TBLB in terms of the percentage of sampled tissue containing open alveoli [10]. The mean maximal diameter of the samples were around 9 mm [15,16]. It was sufficient for histological diagnosis that the samples were larger than 5 mm in diameter as the experts suggestion [17]. Although SLB had been recommended as golden standard for pathological biopsies, the morbidity and mortality limited its clinic performance. A large dataset study showed the rate of in-hospital mortality following SLB for DPLD was 1.7%, the rate of complication was 30% including postoperative pneumothorax, pneumonia, and respiratory failure [18]. Bleeding complications occurred in 22% of patients and pneumothorax was 1.4%. The adverse events during TBLC were significantly lower than during SLB [6,11]. Mortality due to adverse events was observed for 2.7% (SLB) and 0.3% (TBLC) of the patients [18]. In our study, the severe bleeding which prohibited examination was 5.7% and pneumothorax was 2.9%. The advantage of TBLC was more suitable for following and supervising the progressive diseases than SLB owing to less adverse events.
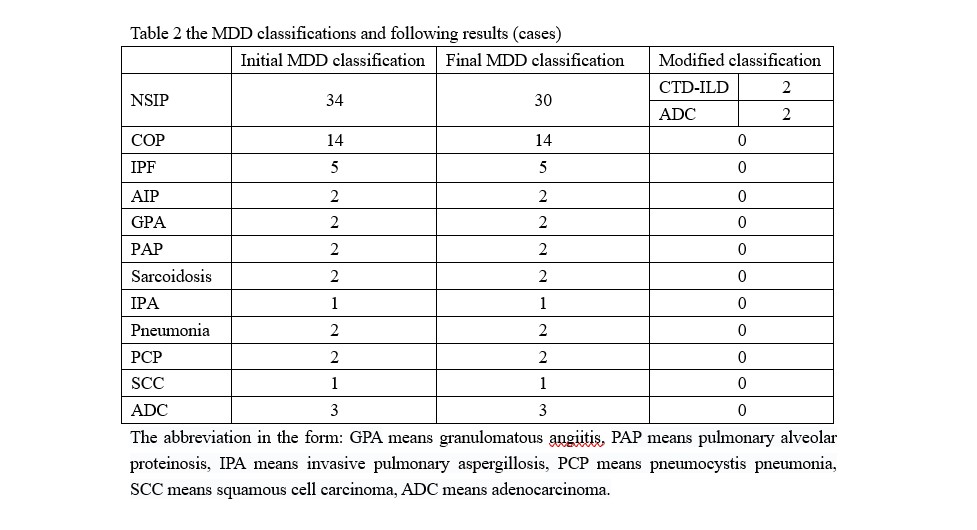
As the gold standard approach for the diagnosis of IIPs, MDD classifications needed to be reached by a multidisciplinary team comprised of expert pulmonologists, pathologists and radiologists after reviewing the available clinical, radiological and pathological data. Clinic and radiological information (from HRCT) alone might lead to typical IPF, cytological or histological information were warranted in others [6, 19]. Tomassetti [20] indicated that the diagnostic confidence was significantly increased depending on the histopathological information from both TBLC and SLB in IPF compared with only clinical-radiological diagnosis. As for DPLD, Ravaglia [21] compared diagnostic yield and showed that the diagnostic pattern was 82.8% in TBLC vs 98.7% in SLB. Kropski [16] and Poletti [18] reported that pathological diagnostic pattern from TBLC was 80%. Ussavarungsi [15] indicated that the definite MDD was yielded in 51% of subjects, and nonspecific histopathologic finding was in 49%. Hetzel indicated that the nondiagnostic rate were about 20% of cryobiopsies [17], the reasons included inadequate lung tissue (the specimen is predominantly airway wall), normal lung tissue (sampling error), or lung tissue with very minor and nonspecific pathology. In this study, the confident diagnostic yield based on transbronchial pathology in IIPs was 77.1%. 94.3% (66/70) initial MDD classifications based on transbronchial pathology was agreed with the final. To follow the therapy was essential for MDD classifications based on transbronchial pathology because 5.7% initial MDD classification was modified.
{kind=link}
{kind=link}