In this nationwide survey of COVID-19 seroprevalence among hemodialysis patients in Senegal, we found that more than one patient in five presented specific antibodies by end of October 2020. Data from previous studies in hemodialysis cohorts reported variable but lower seroprevalences with 2.2% in Wuhan, China [8], 3.3% in France [9], 10.7% in the United Kingdom [10], 14.6% in Brescia, Italy [11], and from 3.5–27.2% in the USA [12]. In a recent review by Kooman JP, et al. the incidence of COVID-19 confirmed by RT-PCR among dialysis patients varied between 0.03% and 19.6% [3].
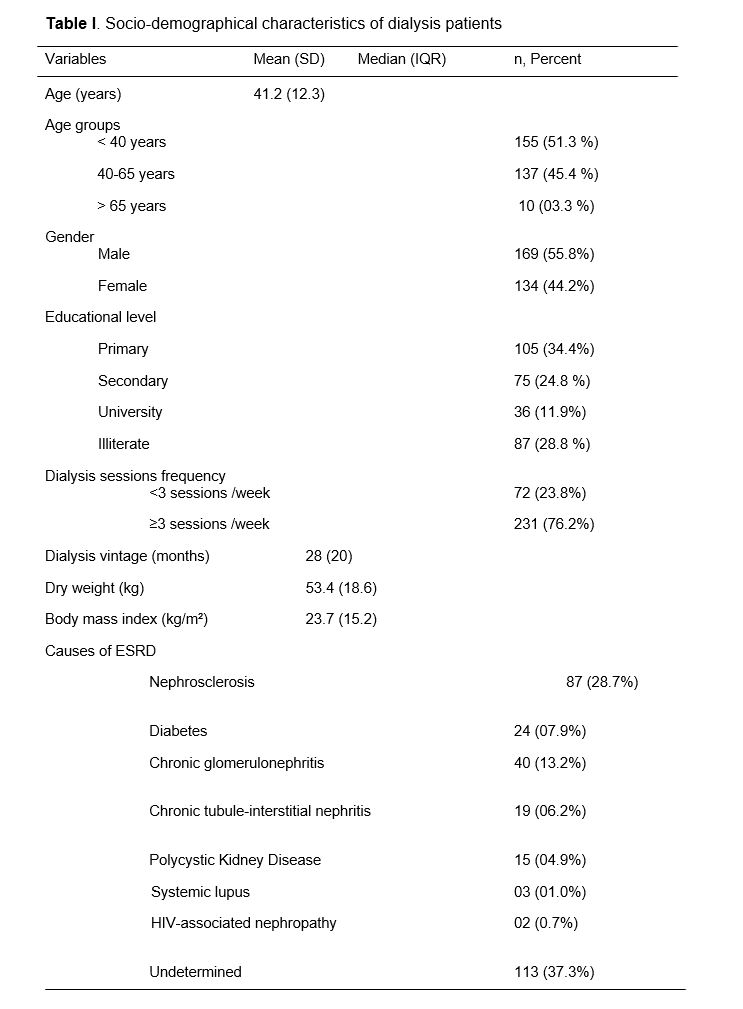
Unexpectedly our patients aged > 65 years showed the highest seroprevalence contrasting with publications where elders in dialysis showed a lower exposition to SARS-CoV-2 but a higher lethality rate [9, 12, 13, 14]. The age structure of the dialysis population in Africa is very different from developed countries where the majority of dialysis patients are 65 years old [9, 10, 11].
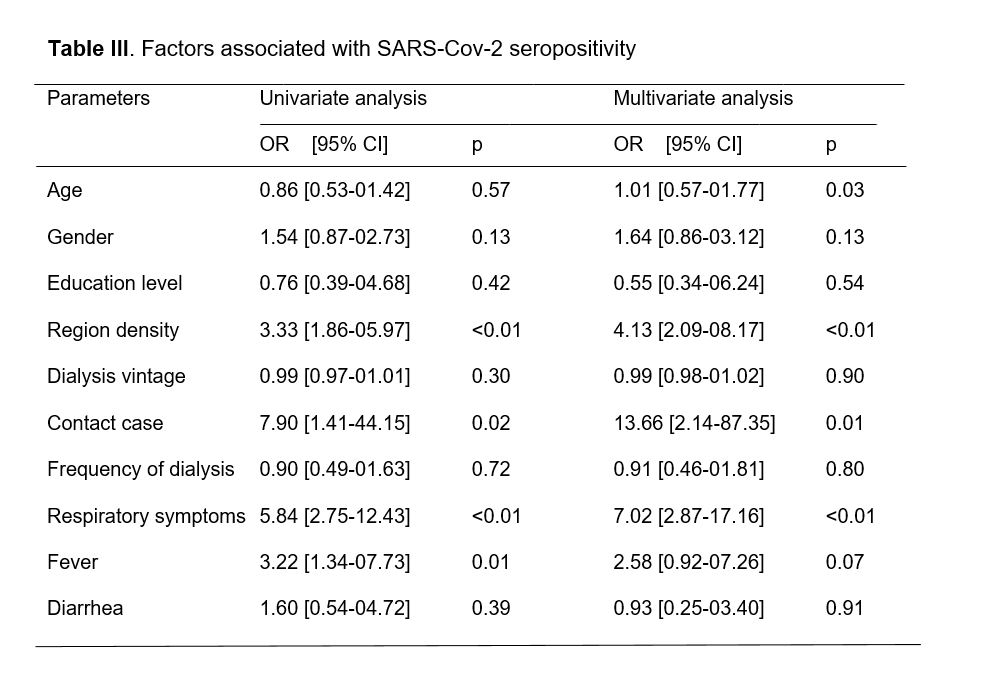
The existence of the previous contact with a COVID-19 case and population density were the strongest factors associated with a positive serology among hemodialysis patients. Regional disparities observed within the country have been also noticed in previous nationwide surveys [9, 12]. They could be explained by the intensity of virus circulation and promiscuity. The regions hosting two-thirds of infected patients were the most densely populated. In these settings, patients used to take crowded public transports to come to dialysis centers. The same hypothesis was evoked by Anand et al in a US nationwide comparative study which found that residents of neighborhoods with high population density presented a ten times higher risk of seropositivity compared with residents of lowest density areas [12]. Since the early pandemic, epidemiological studies suggested that SARS-CoV-2 basic reproduction number (R0) increases linearly with population density [15] and this was why clusters were observed in crowded and confined spaces, mass gatherings, and populous metropolitan areas [16, 17].
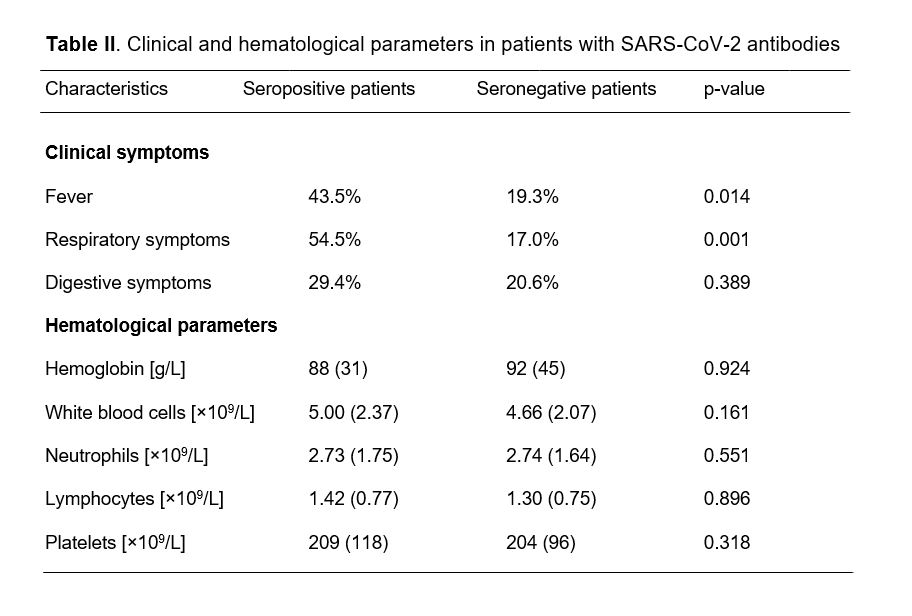
In contrast to the remarkable differences noted between Africa and the rest of the world regarding the extent of COVID-19 in the general population, we found among the hemodialysis subgroup a proportion of patients infected with SARS-CoV-2 which was comparable to data reported in other continents. Some authors suggested that the lower burden of COVID-19 in African countries could be explained by a majority of asymptomatic cases that were not diagnosed [18]. COVID-19 in our hemodialysis patients presented as an asymptomatic disease in 71.9% of cases. Similar to our findings, fever, cough, dyspnea, and fatigue are the most common symptoms described in patients with COVID-19 [3, 19] but digestive or cerebral manifestations can be more prominent in some cases [20].
Many studies using either PCR or serology tests had pointed out the predominance of asymptomatic forms in hemodialysis patients [12, 21] and underlined the paramount importance of preventive measures for all patients and staff inside dialysis centers. Testing strategies focusing on symptomatic cases only are known to underestimate the burden of the COVID-19 as it was demonstrated in the US population during the first wave of the pandemic that fewer than 10% of adults developed antibodies against SARS-CoV-2, and fewer than 10% of those were diagnosed [12]. Furthermore, African populations might develop a slightly different immune system response against the virus modulated by the multiple interactions with environmental factors and pathogens [22, 23].
Routine full blood count did not show any specific abnormalities in our patients with positive serology contrasting with data general population where one in four COVID-19 patients presented leukopenia (WBC < 4×109 cells/L) and lymphocytopenia (lymphocyte count < 1×109 cells/L) was found in 63.0% of them [13]. Albalate M, et al reported lymphopenia in almost half of the dialysis patients with confirmed COVID-19 [21]. Various hematologic features were reported in patients with COVID-19 but hyperleukocytosis, lymphocytopenia, and thrombocytopenia might be correlated with disease severity [24]. The absence of such hematologic perturbations in this study is concordant with the low COVID-19 related morbidity and mortality rates observed in our patients who rarely presented with severe forms of the disease requiring admission at intensive care units.
This mortality rate of less than 1% among Senegalese hemodialysis patients is following relatively fewer deaths reported in African populations since the first pandemic wave [4, 18]. However, emerging data suggest a more deadly second wave with a 40% increase in deaths in the continent since January 2021 [25]. Studies in other continents showed a mortality rate between 20% and 32.8% in hemodialysis patients with COVID-19 [25, 27, 28]. The younger age in our cohort was the main explanation for the lower number of deaths despite a higher incidence of COVID-19 cases.
In absence of seroprevalence data in the Senegalese general population, our findings in this representative nationwide hemodialysis cohort could serve as a good proxy to guide decisions of health authorities in the elaboration of an evidence-based strategy against COVID-19. Hemodialysis patients represent a good sentinel population in which to study the evolution of the current pandemic. Because we performed a serological test using blood samples collected as part of routine medical care, our results might not be influenced by possible selection bias compared to other previous studies that used nasal swab RT-PCR tests usually reserved for symptomatic patients.
Thus, these data in hemodialysis patients present a great epidemiological interest because it can be linked to community-level data to enable evaluation and quantification of differences in SARS-CoV-2 prevalence across socio-demographic and geographical strata, and thus develop efficient strategies targeting the highest-risk groups and areas.
Recent immunological studies demonstrated that patients with mild COVID-19 forms might develop multipotent SARS-CoV-2-specific immune memory response and IgG antibodies against spike protein could persist after recovery at least for three to six months [29, 30]. By demonstrating that many hemodialysis patients had already evidence of exposure and developed an immune response to SARS-CoV-2, this study opens prospects for future vaccination strategies in this specific group. The rationale of mass vaccination without excluding recovered patients with enough SARS-CoV-2 Ig G is yet to be demonstrated and benefits should be balanced with possible side effects and costs particularly in hemodialysis patients [30].
Limits
Although we used a large and representative sample of dialysis patients in Senegal, our study presents some limits. First, the antibodies IgM and IgG are detected day 3–7 days after a person is infected by SARS-CoV-2 which suggests the serology test used may miss early infected people. Secondly, the retrospective collection of clinical symptoms and routine biological analysis could induce some recall bias when information was not written in the patient medical record. Also, we did not have some socio-demographical parameters like employment status, income level, living space, household size, and type of transportation from house to the dialysis center that could influence patient’s risk of contamination. However, the current results in this sub-group of dialysis patients might not reflect the true estimates in the general population. These results probably underestimate overall seroprevalence because dialysis patients usually face restrictions in their socio-professional activities due to their condition and maybe less in contact with the general population [31, 32]. Furthermore, data from hepatitis B post-immunization studies had demonstrated that compared to the general population, patients receiving dialysis might have a weaker immune response to viral antigen and thus be less likely to develop protective antibodies [33].
Finally, the early release and implementation of national guidelines for prevention and control of COVID-19 cases in dialysis facilities might have reduced the risk of in-center infections among patients and health workers.
{kind=link}
{kind=link}
{kind=link}