As a BRAF inhibitor, vemurafenibis is superior to chemotherapy concerning PFS, OS, and ORR, in BRAF mutant advanced melanoma patients (22). A second BRAF inhibitor, dabrafenib, exhibited a significantly way to improve PFS, compared to chemotherapy (23). Compared to BRAF inhibitors, the MEK inhibitors trametinib and binimetinib had lower ORR (20 vs 50%); however, they were more superior, compared to chemotherapy in patients with BRAF-mutant advanced melanoma (24, 25). The majority of patients treated with BRAF or MEK inhibitors develop drug resistance. Combining BRAF and MEK inhibitors may overcome this limitation. The superiority of combining these two inhibitor categories, compared to single-agent inhibitor therapy, was confirmed in several randomized trials, with PFS rate of 19% and OS, 34% at 5 years of receiving dabrafenib plus trametinib (26); mPFS, 14.9 months and mOS, 33.6 months receiving encorafenib plus binimetinib (27); mPFS, 9.9 months and mOS, 22.5 months receiving vemurafenib plus cobimetinib (28); and mPFS, 10–14 months and mOS, about 24 months (29). BRAF and MEK inhibitor combination improves outcomes in melanoma patients, with high adverse event frequencies. Moreover, resistance occurs eventually. Because of this, other molecular-targeted strategies are also being studied, including the use of small-molecule tyrosine kinase inhibitors of VEGF.
In the present study, apatinib showed antitumor activity in patients with malignant melanoma, with median PFS and OS of 4.0 and 12.0 months, respectively. Univariate analysis showed that several baseline factors (sex, age, subtypes, lactate dehydrogenase level, number of organ sites, with metastasis, and treatment lines) were not associated with either PFS or OS. Although not as good as BRAF and MEK inhibitors, considering that the patients enrolled are on second-line treatment, the drug has certain prospects and is worthy of large-scale clinical studies in malignant melanoma.
The toxicity profile was generally consistent with prior results using apatinib in a phase I study, with the safety data of other multi-kinase inhibitors of the same class. The adverse events were hypertension, hand-foot skin reactions, canker sores, liver function damage, hemorrhage, diarrhea, sick, anepithymia, rash, and fever. Most of these adverse events were mildly graded. Only a small proportion of subjects reported grade 3/4 events. Among these, one patient (6.67%) had grade 3 hypertension and one (6.67%), grade 4 canker sores.
Apatinib efficacy and safety in this study were consistent with a prospective phase I study launched by Guo’s team (30). In that study, 12 patients were treated with various apatinib doses (250 or 500 mg daily) plus temozolomide (100 or 200 mg). Among them, 1 patient achieved PR and 9 achieved SD. The ORR was 8.3% and DCR was 83%. mPFS was 3.3 months and mOS 6.3 months. Regarding safety, dose-limiting toxicities were not observed even in the temozolomide 300 mg plus apatinib 500 mg daily group. In a retrospective analysis of 22 patients treated, with 500 mg apatinib per day, ORR was 9.1% and DCR 59.1%. The mPFS was 7.5 months (31). The common feature of these two studies and ours is that the patients enrolled are Chinese, with mainly malignant melanomas of the mucosa and extremities. These two types of malignant melanoma have a low BRAF gene mutation rate; therefore, they may not be sensitive to BRAF inhibitors and PD-1 antibodies (32). Therefore, anlotinib may have better application prospects in this population.
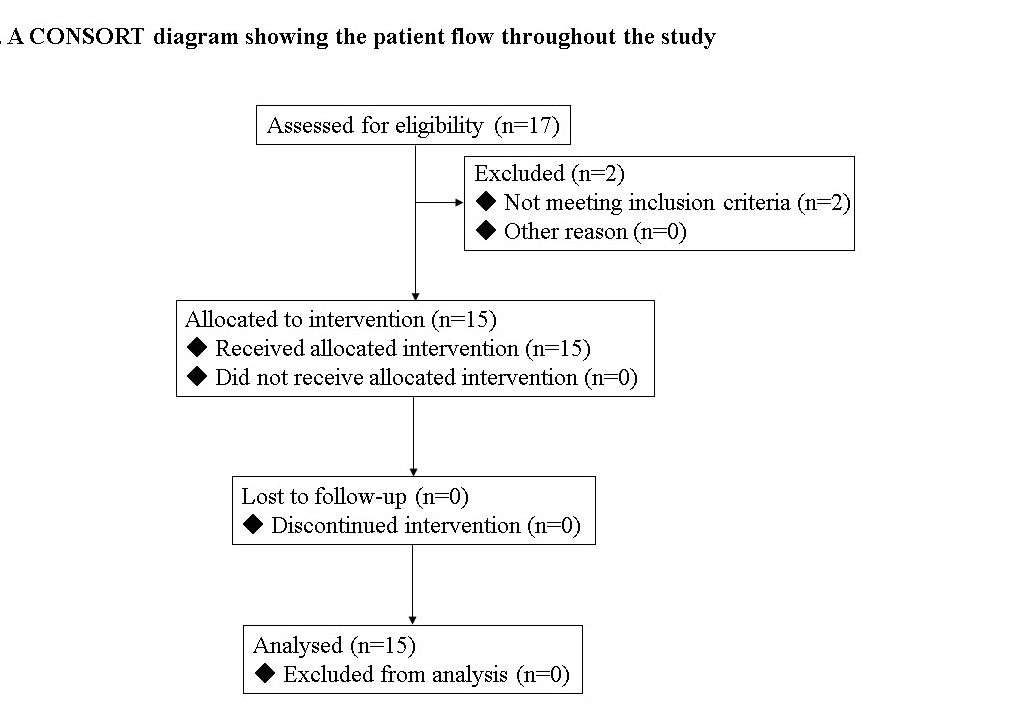
The present study had some limitations. When the IIT study was designed, vemurafenib or PD-1 mAb had not been approved for use in Chinese melanoma patients, and dacarbazine-based chemotherapy was the first-line treatment. Therefore, the initial inclusion criteria consisted of treating chemotherapy-refractory melanoma patients with first-line therapy. However, with vemurafenib and PD-1 approval in melanoma in China subsequently, patients had more standard choices. It became difficult to enroll new patients, who receive only the first-line treatment. After careful discussion, the study investigators and sponsor revised our regimen, according to the applicable regulations, protecting the rights, safety, and welfare of subjects. Consent was obtained from patients with second-line or above treatment. Eventually, 15 patients were analyzed in the study, among which 9 had first-line treatment and 6 had second-line or above treatment. Additionally, the patients enrolled in this study were from China. The generalizability to other populations remains unclear. Finally, due to the small sample size of this study, the results we have obtained on patient prognosis are not significantly correlated, with baseline data and need to be interpreted with caution.
{kind=link}