PACNS is an uncommon single-organ vasculitis that is still poorly understood(9-11). PACNS could lead to various neurological manifestations, including headache, altered cognition, focal weakness, and stroke(1). The three different pathology types of PACNS are granulomatous, lymphocytic, and necrotizing vasculitis, of which granulomatous vasculitis is the most common, featuring vasculo-centric mononuclear inflammation and well-formed granulomas with multinucleated giant cells(1, 12). Diagnostic criteria for PACNS were first proposed by Calabrese et al., which has been widely used for over 20 years, and consist of the following: (1) the presence of an acquired otherwise unexplained neurological or psychiatric deficit; (2) the presence of either classic angiographic or histopathologic features of angiitis within the central nervous system; and (3) no evidence of systemic vasculitis or any disorder that could cause or mimic the angiographic or pathologic features of the disease(7). Nevertheless, diagnosing PACNS can be quite challenging because of its diverse clinical features and lack of crucial laboratory tests. Most of the mimicking conditions would not benefit from steroids and immunosuppressive therapy, so the accurate diagnosis is very important. Brain biopsy is still the gold standard and should be performed whenever possible. But due to the invasive nature of biopsy, it has its limits, especially for intracranial vessels(13).
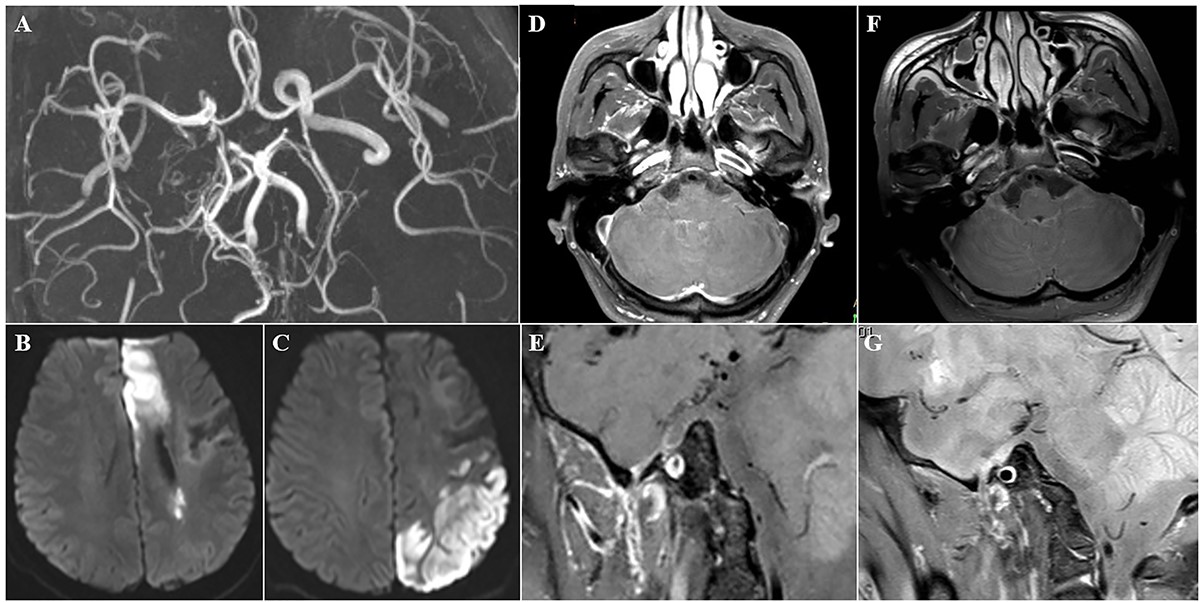
Several vasculopathies, such as reversible cerebral vasoconstriction syndrome (RCVS), atherosclerosis, moyamoya disease, and fibromuscular dysplasia, could show similar imaging features as PACNS on traditional imaging protocols like CTA、MRA or DSA, showing “beading” pattern of segmental dilation and narrowing of multiple cerebral arteries(2, 14-16). VW-MRI could directly visualize the abnormality of the vessel wall and therefore has become an important tool for evaluation. Vasculitis is usually characterized as smooth, homogeneous, concentric arterial wall thickening with enhancement, while atherosclerotic plaque usually displays nonconcentric and heterogeneous vessel wall abnormality. RCVS can show similar smooth, concentric vessel wall thickening with or without diffuse vessel stenosis. But patients with RCVS would not display vessel wall enhancement(17-20). Furthermore, in order to precisely interpret VW-MRI images, the images need to be analyzed in at least both long-axis and short-axis plane. But for 2D VW-MRI sequences, they can only be restricted to one fixed angle for one time scanning process(Add Fig 4D-F). Since the intracranial vessels can be oblique, curved, and tortuous, 2D sequences could lead to partial volume averaging effects and confound the vasculopathies(6, 20). Since the 3D VW-MRI sequences we applied are isotropic, they can be reconstructed in any angle. Additionally, 3D isotropic VW-MRI sequences with a big field of view including both the complete brain vasculature as well as the cervical arteries can supply images more efficiently, with relatively less artefacts, in relatively less time, since they are more stable against laminar flow and other artifacts(21-23). Several previous studies had illustrated that 2D VW-MRI can be a valuable approach to differentiate various vasculopathies, as well as provide more precise evaluation of vessel wall(3-5, 17, 24-31). The application was also recommended in the “ Intracranial Vessel Wall MRI: Principles and Expert Consensus Recommendations of the American Society of Neuroradiology(20)”.
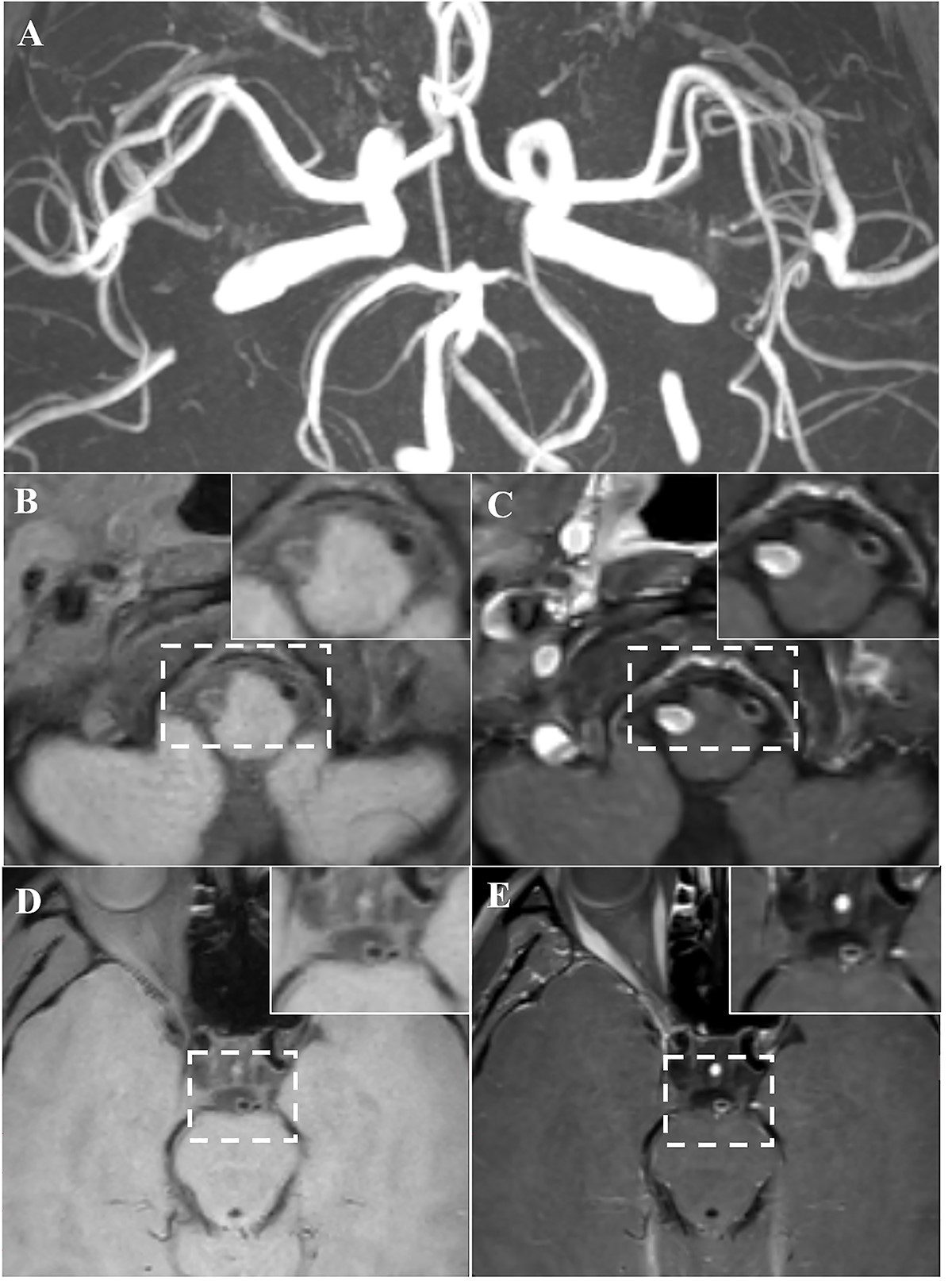
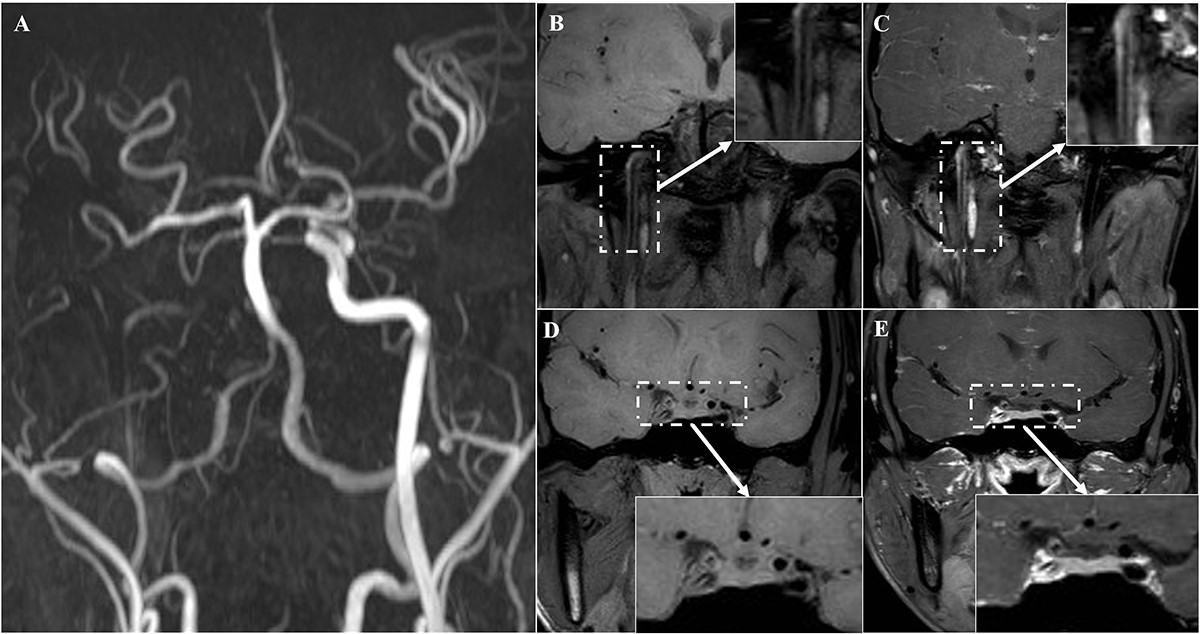
In this study, we present 5 cases of PACNS that including 13 affected vessels. We speculate that cervical arteries are more vulnerable to PACNS; meanwhile, due to the existence of vasorum, the interpretation of cervical artery vessel wall enhancement needs to be done cautiously, since they might be a normal phenomenon of vasa vasorum enhancement. There were 13 involved vessels in these 5 cases. With regard to vessel wall thickening and enhancement pattern, 12 (12/13, 92.3%) vessels showed circumferential or eccentric wall thickening with contrast enhancement, and only 1 (1/13, 7.69%) vessel displayed absence of vessel wall thickening or enhancement on admission, but showed progression on follow-up observation. Among the 12 vessel wall enhancements, 11 (11/12, 91.7%) showed homogeneous enhancement pattern, 1 (1/12, 8.3%) showed eccentric enhancement. As for the degree of vessel wall enhancement, 1 (1/12, 8.3%) showed grade 0 intensity, 2 (2/12, 16.7%) showed grade 1 intensity, and the other 10 (10/12, 83.3%)vessels showed grade 2 intensity (Tab 1). Furthermore, all the 5 cases were involved of both anterior and posterior circulation, even the vasculopathy may be asymptomatic. Compared with traditional 2D VW-MRI, 3D isotropic VW-MRI could assess the whole brain and neck vasculature in one time, and apple reconstruction in any angle. It would be more convenient since PACNS can be multiple-vessel-involving.
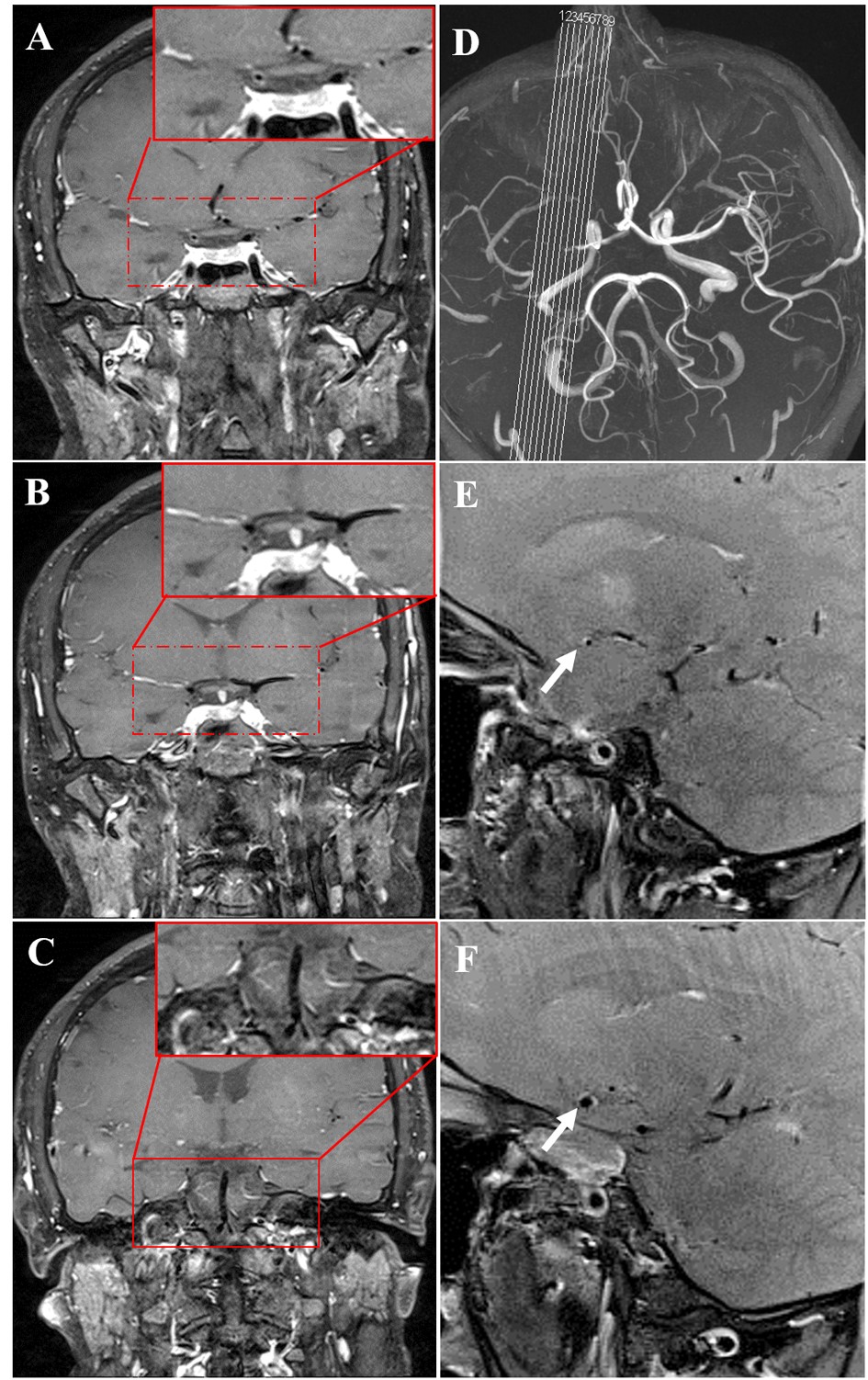
To our knowledge, there were three articles that described follow-up features of PACNS. Pfefferkorn et al described moderate-to-strong enhancement in 4 patients with PACNS. As for follow-up, 2 patients showed persistent vessel wall enhancement on 2 months and 2 patients displayed resolution of vessel wall enhancement on 6 months, all of them were given immunosuppressive therapy(25). The second case report by Saam et al described a patient diagnosed of PACNS with strong vessel wall enhancement in multiple arteries. Follow-up imaging showed partial resolution in vessel wall enhancement on 3 months, and further substantial decrease with some persistent enhancement on 6 months(32). E.C. Obusez et al reported 13 PACNS patients with temporal patterns, the vessel wall thickening and enhancement were persistent for a median of 13.5 months in 4 patients. While in other 2 patients, there was complete resolution after a mean of 7 months(5). In our study, five patients separately took steroids, immune-suppressors, antiplatelets, and parahormone therapy, and three patients completed the imaging follow-up at 3-24 months. One patient displayed partial resolution on 3 months of steroids; one patient showed persistent vasculopathy at 24-month follow-up, the other patient (Case 1) showed gradual resolution of the anterior circulation but progression of the posterior circulation. Especially for case 1, the left vertebral artery of the patient was normal on disease onset, while saw gradual occlusion in 12 months.(Fig 1, Tab 2). The findings in our study were consistent with previous researches, reminding us of the stubborn and aggressive nature of PACNS, as well as the importance of whole brain and neck vasculature evaluation. Our case series had several deficiencies, including the absence of brain biopsy evidence and incomplete imaging follow-up. But we do explore the utility of 3D isotropic VW-MRI in PACNS.
We assert that 3D isotropic VW-MRI can evaluate the specific vasculopathy as well as the whole brain vasculature more effectively. 3D isotropic vessel wall imaging could evaluate the specific responsible vessel as well as the whole brain vasculature in one-time scan, providing detailed information in detection, diagnosis, evaluation and follow-up. Moreover, primary angiitis of the central nervous system tend to be multi-vessel involving, so the 3D isotropic vessel wall imaging could be more applicable. Thus far, the application of imaging in PACNS was qualitative. In the future, as the improvement of 7 Tesla scanning techniques, VW-MRI may achieve quantification assessment of vasculitis and provide more utility for PACNS(33).
{kind=link}
{kind=link}
{kind=link}
{kind=link}