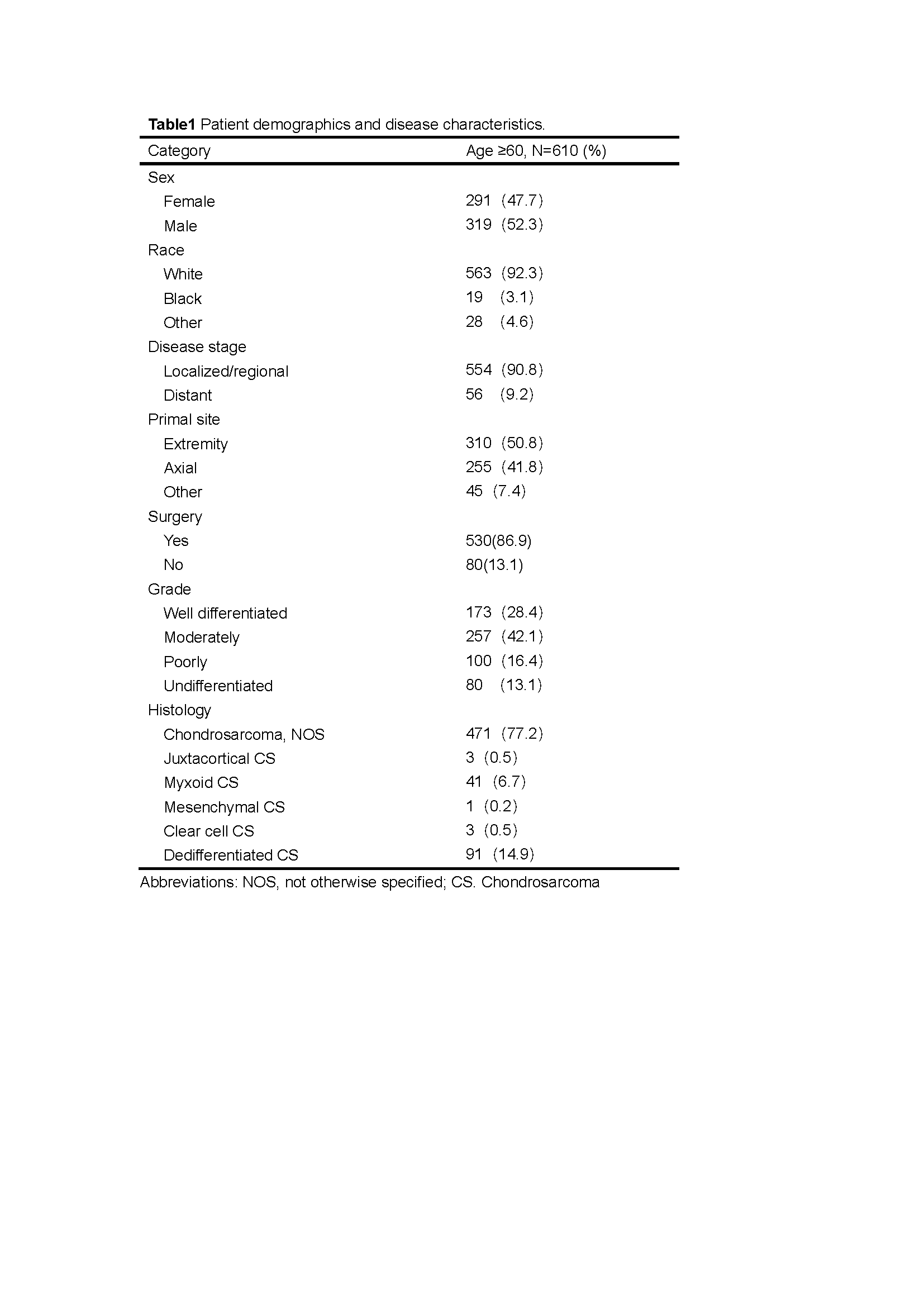
Chondrosarcoma is the second common malignant tumor of bone after osteosarcoma. In general, conventional chondrosarcoma is a disease more commonly found in adults range from 40 to 60 years old. It is also the most common bone sarcoma in the elderly.9; 10Few specific studies had been conducted on chondrosarcoma patients over 60 years of age. Meanwhile, the number of elderly people in the world is increasing, and the number of cases of chondrosarcoma will increase correspondingly. In this study, we performed a survival analysis in patients with chondrosarcoma older than 60 years in order to identify the prognostic factors and guide the clinal treatment based on SEER database.
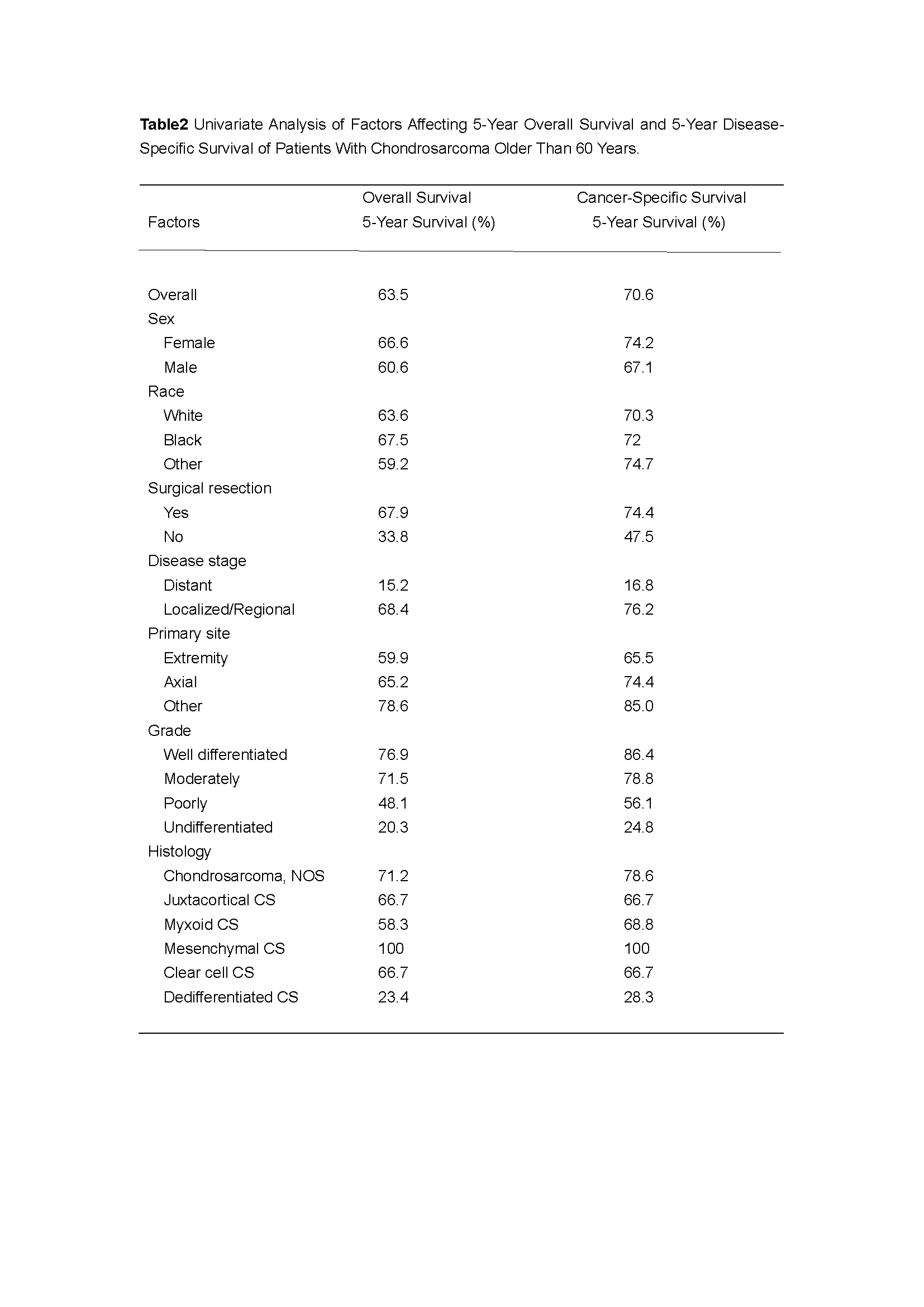
Overall survival (OS) and cancer-specific survival (CSS) were analyzed in this 610 cases older than 60 years old. Our research shows that overall survival and cancer-specific survival were 69.3% and 74.4% at 3 years, 63.5% and 70.6% at 5 years, and 52.3% and 63.5% at 10 years. Timothy A. Damron had reported that the five-year survival rate for chondrosarcoma is 75.2% based on 9606 cases from the National Cancer Data Base of the American College of Surgeons.11The reason our results are lower is that age is a strong prognostic factor, as confirmed in Julian Fromm and earlier studies.12
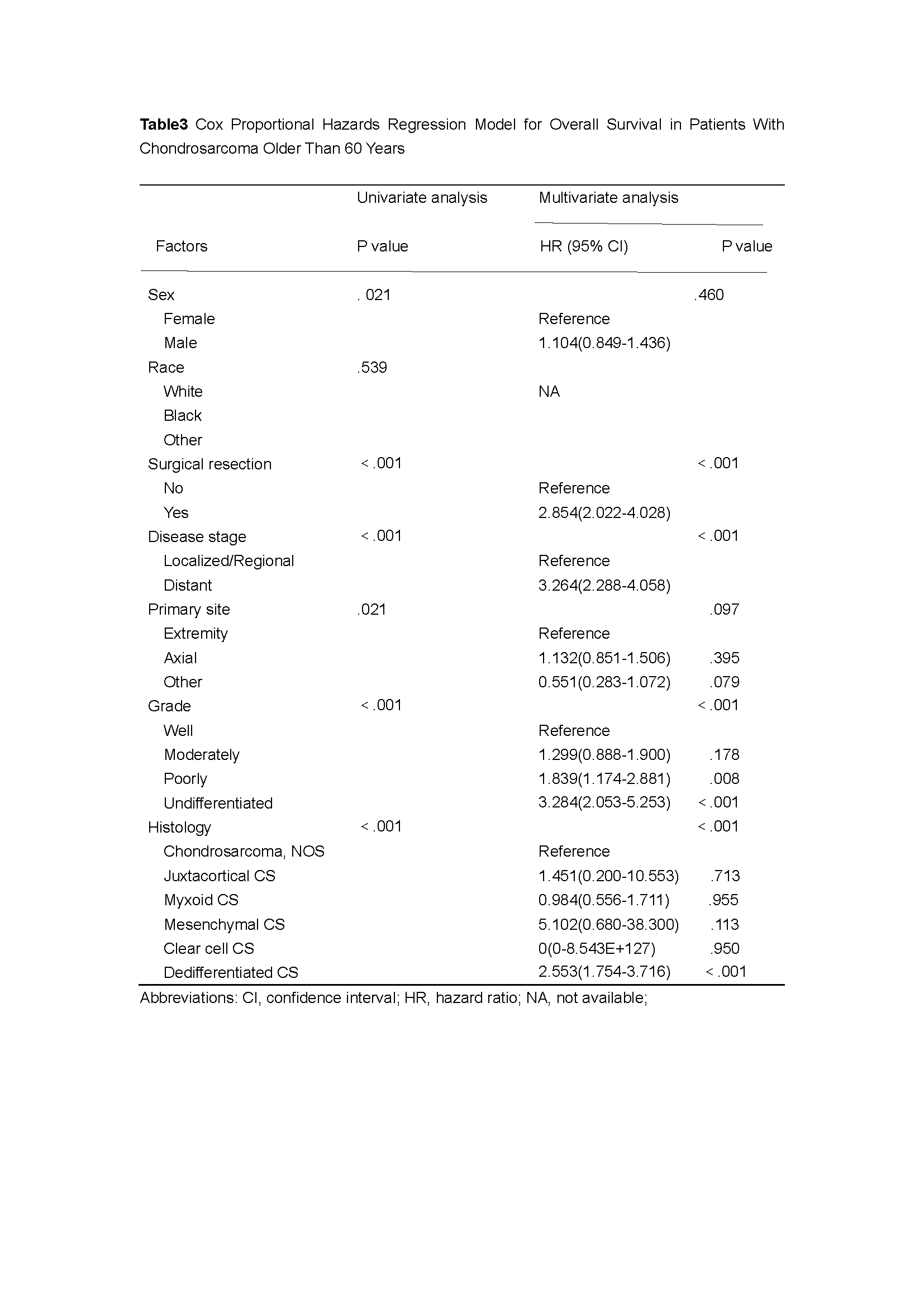
Undoubtedly, surgical resection is an important prognostic factor. Surgery is the foundational treatment strategy for chondrosarcoma, on the purpose of preserving or even improving functionality, relieving pain, controlling local recurrence, and promising prolonged survival. One of Douglas J. Pritchard’ studies about 280 chondrosarcoma patients who had seen at the Mayo Clinic showed that those who had surgical recession had far fewer relapses than those who had not. Similarly, M. K. Laitinen reported that wide local excision plays an important role in 126 chondrosarcoma patients with local recurrence of the pelvis and limbs.13–15 Of course, Specific surgical methods is determined based on stage, grade, and location. Unfortunately, specific information on the type of surgery performed and the adequacy of surgical margins is not included in the SEER database.
It is commonly believed that the primary site has a certain influence on the prognosis of chondrosarcoma. It occurs more in the central skeleton, commonly arising from the pelvic girdle, vertebrae, and proximal long bones4 The site of origin may affect outcome in chondrosarcoma, with some anatomic locations such as the pelvis known to predict a worse prognosis than others. This may be due to differences in biological behavior, or may reflect the difficulty achieving an R0 resection in these locations. 16For example, Those tumors which crossed the sacroiliac joint had a higher incidence of local recurrence compared with those at other sites. As D. Donati analysed, the inaccuracy of estimating the degree of tumor extension across the sacroiliac joint, as well as the difficulty in performing the bony cuts during resection combined with tumor infiltration into the sacral wing, explains the higher incidence of inadequate margins and local failure in these patients. 17In Axial chondrosarcomas(including pelvic and spine), published 10-year survival rates vary between 52 and 80 %12; 17–20 While in extremity, published 10-year survival rates range from 69–81%17; 21. Surprisingly, our study demonstrated that univariate Cox regression analysis of Survival for the anatomical site is significant (P = 0.021) while multivariate Cox regression analysis was not(P = 0.097). One of the possible explanations for this inconsistency is the primary site of the tumor was not subdivided in our study. Confounding factors affected the accuracy of the results.
In this study, we confirmed that metastasis and higher grade suggested poor prognosis, which had been reported in many previous studies. High grade chondrosarcomas have a higher incidence of distant metastasis which made a bad influence on surgical methods and results. 17 Shuting Bai showed that the CXCR4 expression was detected in both the cytoplasm and nucleus of the chondrosarcoma and nonneoplastic cartilage cells. CXCR4 expression levels increased in high-grade chondrosarcoma cells compared with low-grade specimens. high-grade tumor cells show greater CXCR4 expression. This may account for the difference in survival between high-grade and low-grade chondrosarcoma. 22The metastasis of chondrosarcoma is predominantly hematogenous. Distant metastases to the lung are the most common, followed by skin and soft tissue. The rate of metastases has been also found higher in pelvic and chest wall chondrosarcomas, compared to conventional chondrosarcomas of the extremities Metastatic chondrosarcomas has a better postoperative recurrence rate.21; 23
The present study has several limitations. Firstly, the SEER database does not contain specific surgical information which had been known as potential prognostic factors including pathologic fracture, surgical margin status, radiotherapy, and chemotherapy incomplete.24 Secondly, this is a retrospective study. Thirdly, Under strict inclusion and exclusion criteria, our study had eliminated a lot of unknown and blank information, this would lead to the reduction of other eligible cases and thus magnify the statistical difference. Still, the SEER database has a significant advantage in studying rare tumors.
{kind=link}
{kind=link}
{kind=link}