Population and region-specific interventions are required to achieve global elimination as contextual factors vary across place and sub-populations. Our study provides an in-depth understanding of the prison TB epidemiology, together with its interaction with the HIV epidemic, at the Kality Federal Prison, Ethiopia during 2009–2017. As the Kality Prison is not only a long term detention center but also a short term detention center, it can transmit the TB infection to the general population through short term prisoners upon release and to other federal prisons when inmates are transferred from Kality Prison (13).
The trends analyses indicated that over time the TB epidemic has evolved within the prison setting with implications for TB control and prevention management. The proportion of EPTB and microbiologically confirmed PTB increased over time while TB-HIV coinfection declined over the course of the study. These data suggest that the TB control strategy for this prison population should be refocused to include traditional, as well as non-traditional risk groups especially based on age, previous TB diagnosis and finer TB categorizations as discussed in detail below.
The increase in microbiologically confirmed cases of PTB might suggest increased risk of transmission within the prison, disease severity due to delayed diagnosis/treatment or reactivation due to prison conditions, raising concern over existing TB prevention/control strategies. A recent study of the Kality Prison in Ethiopia documented that the prevalence of bacteriologically confirmed PTB (BC-PTB) was higher among jail residents compared to jail entrants, suggesting increased risk of intramural transmission or reactivation of pre-incarceration acquired PTB due to stressful prison environment (13).This increasing trend is consistent with the national trend (Supplementary Fig. 1), but it is possible that these trends are reflective of changes in diagnostic practices or roll out of interventions such as Heal TB aimed at improving case detection among inmates that occurred between 2011–2016 (14).
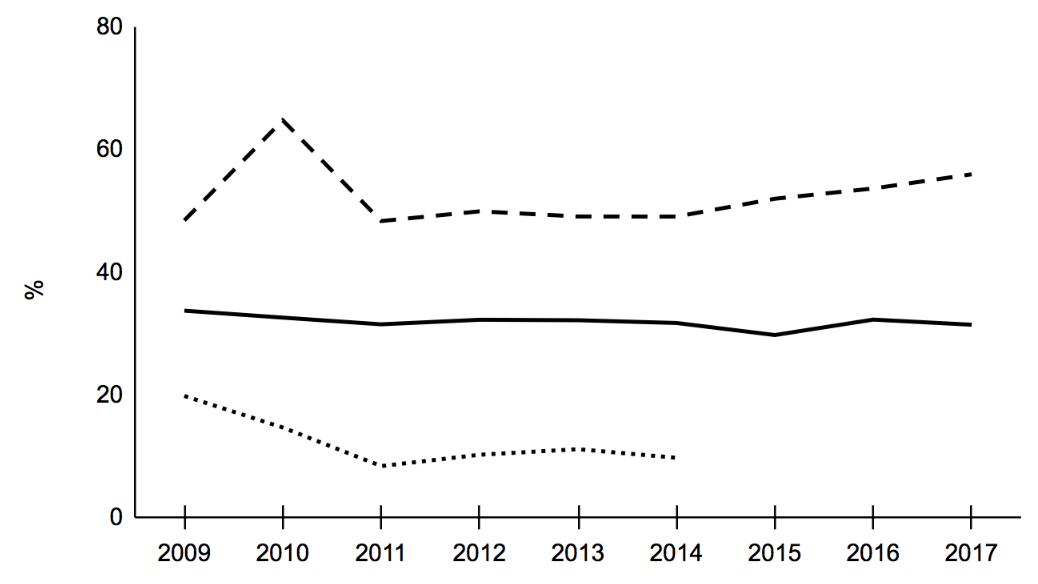
The extrapulmonary TB cases expressed as a percentage of total new/relapse cases is indicated by the solid line, the microbiologically confirmed pulmonary TB cases expressed as a percentage of pulmonary TB cases are indicated by the dashed line and HIV seroprevalence among those with a recorded HIV test result is indicated by the dotted line.
Our results, although not statistically significant, suggest a 3% increase in the proportion of microbiologically confirmed PTB among 18–24 year age group, ranging between 26% reduction and 43% increase in the likelihood of microbiologically confirmed PTB (aPR = 1.03; 95% CI: 0.74, 1.43). These findings may suggest lack of timely diagnosis and underutilization of medical services among this group as 80% of the microbiologically confirmed cases in our study had a positive sputum smear result. Hence, control strategies should be focused towards these younger inmates that are presumably more likely to spread the infection as sputum positive patients tend to be more infectious compared to only culture positive patients (15, 16). We chose to not discredit observed effect estimates in this study solely based on p-value threshold while also acknowledging the associated uncertainty because absence of statistical significance alone does not prove the null hypothesis (17).
A resurgence of EPTB is largely attributed to the HIV epidemic in high burden countries (18). However, in our study, the proportion of EPTB cases increased over the course of the study period while the HIV coinfection proportion declined. The HIV seroprevalence among TB patients was many folds higher among the prisoners compared to the national estimates as noted by other studies as well (19–21) (Supplementary Figure). A prior study conducted among newly diagnosed HIV patients in Addis Ababa found the coinfection percentage to be 7% (22). It appears that HIV management among TB patients is driving down TB-HIV trends, while EPTB trends are likely driven by factors other than HIV as our study did not find HIV patients to be at an increased risk of EPTB (aPR = 0.73, p-value = 0.03). HIV management in Ethiopia has shifted from focusing on only those with AIDS diagnosis to testing and treating every HIV-positive case to ensure earlier access to anti-retroviral treatment. However, our sensitivity analysis (Supplementary Table) revealed that EPTB patients were more likely to have a missing HIV test result in our study (aPR = 1.94, p-value < 0.01). If HIV sero-positive individuals among EPTB patients were more likely to not have a record for a HIV test, then it may explain the lower likelihood of EPTB among HIV positive patients compared to HIV negative patients.
Additionally, our study reported that young age (18-44 years) was associated with increased risk of EPTB as compared to the older age group, although only marginally significant (p-value=0.06). Contrary to our finding, prior studies have reported that old age is associated with EPTB (23,24). This unique finding again reiterated the importance of studying the local context as traditional risk factors do not seem to explain the EPTB increasing trends. Similarly, age does not seem to alter the risk of HIV co-infection in a traditionally reported manner as the youngest group between 18-24 years experiences lower risk of coinfection compared to those over 45 years (25).
Prisoners having a previous TB diagnosis were more likely to have HIV coinfection, similar to earlier studies (26). In our study, those who defaulted, failed treatment or relapsed after receiving initial TB treatment were encoded as previously diagnosed TB patients. TB-HIV coinfected individuals often experience pill burden and adverse drug-drug interactions that complicate TB treatment, causing low adherence among coinfected individuals (27).
Similar to a number of previously published studies, this study also highlights the importance of resolving the TB epidemic based on its various manifestations/presentations including EPTB, microbiologically confirmed PTB, clinically diagnosed PTB and TB-HIV coinfection given that each of these TB manifestations are differentially associated with various risk factors (28,29).
Although a previous study was conducted at the Kality Federal Prison as mentioned earlier (13), our work extends the understanding of TB epidemic among Ethiopian prisoners and adds to the existing literature on prison TB by including additional analyses of clinically diagnosed PTB and EPTB cases and using a much larger number of BC-PTB cases (243 vs. 22). Our study additionally assessed trends of prison TB at Kality Federal Prison to track how the TB program has performed over time while also identifying risk factors associated with EPTB, microbiologically confirmed PTB and TB-HIV coinfection. We also provide adjusted prevalence ratios (aPR) using log binomial regression rather than prevalence odds ratios (POR) from a logistic regression as PR is more interpretable and a better estimate of the true effect when the outcome is not rare (30,31).
However, our study also had several limitations. First, due to the use of cross-sectional data, we were unable to establish a cause and effect relationship between risk factors and outcomes. We were also unable to provide incidence estimates as total population estimates for the prison were not available. The trends described in this are, therefore, not only reflective of new cases but also previously treated cases. However, 94% of the cases were new/relapse while the remaining had been previously treated or had unknown TB history. The incompleteness of data for HIV test result and comorbidity may have resulted in selection bias and residual confounding respectively.
{kind=link}