Head and neck carcinoma (HNC) is the sixth most common malignancy worldwide (1), including cancers at oral cavity, pharynx, larynx, paranasal sinus, and so on. Most of head and neck carcinomas are squamous cell carcinoma, although a small amount of them are basaloid squamous cell carcinoma, verrucous carcinoma or other types of cancers (2). According to the statistics, there are over 650,000 new cases of HNC and 35,000 deaths every year (3), most of which are at advanced stage with regional lymph node or even distant metastases (4). In addition, the 5-year survival rate of HNC still remains less than 50% (5–7), which is even worse when HNC is at some specific locations like hypopharynx (8). The conventional treatment strategy for HNC is composed of surgery, chemotherapy and radiotherapy. Recently, immunotherapy and combined therapy are emerging for HNC. However, there are still considerable amounts of patients who don’t benefit from the treatments aforementioned. And the specific anatomic locations of HNC and the treatments often result in the damage in speaking, chewing, swallowing, or even breathing, impairing the prognosis of the patients (9). Thus, it is still a must to study further the mechanisms of the carcinogenesis and progression of HNC.
Inflammasomes play an vital role in responding to insults either externally or internally, assembled with nucleotide-binding domain and leucine-rich repeat-containing (NLR) proteins or absent in melanoma 2 (AIM2)-like receptors (ALR), mainly including NLR family CARD domain containing 4 (NLRC4), NLR family pyrin domain containing 1 (NLRP1), NLPRP3, AIM2, and so on (10). It activates caspases 1, 11 or 8 (11–13), promoting the production and release of pro-inflammatory cytokines IL-1β and IL-18 and the cell death (12, 14, 15). What’s more, not only are inflammasomes expressed in inflammatory cells, but also capable of initiating inflammatory responses in the cells, like gingival epithelial cells infected by Porphyromonas gingivalis in the oral cavity, producing IL-1β and IL-18 as well (16). And the disturbance of inflammasomes is related with various types of diseases (10, 17), including cancers (13, 18, 19). Among them, inflammasomes are also linked with head and neck cancers. However, although it is reported that some inflammasomes were upregulated in certain kinds of head and neck cancers (20), indicating a poorer prognosis (21), some were unchanged (22) and others even were favorable prognostic markers (23, 24). They may have contradictory functions in promoting antitumor immuno-microenvironment and triggering oncogenic activities (23). These together show us that the roles of inflammasomes in the prognosis of head and neck carcinomas are not illustrated clearly.
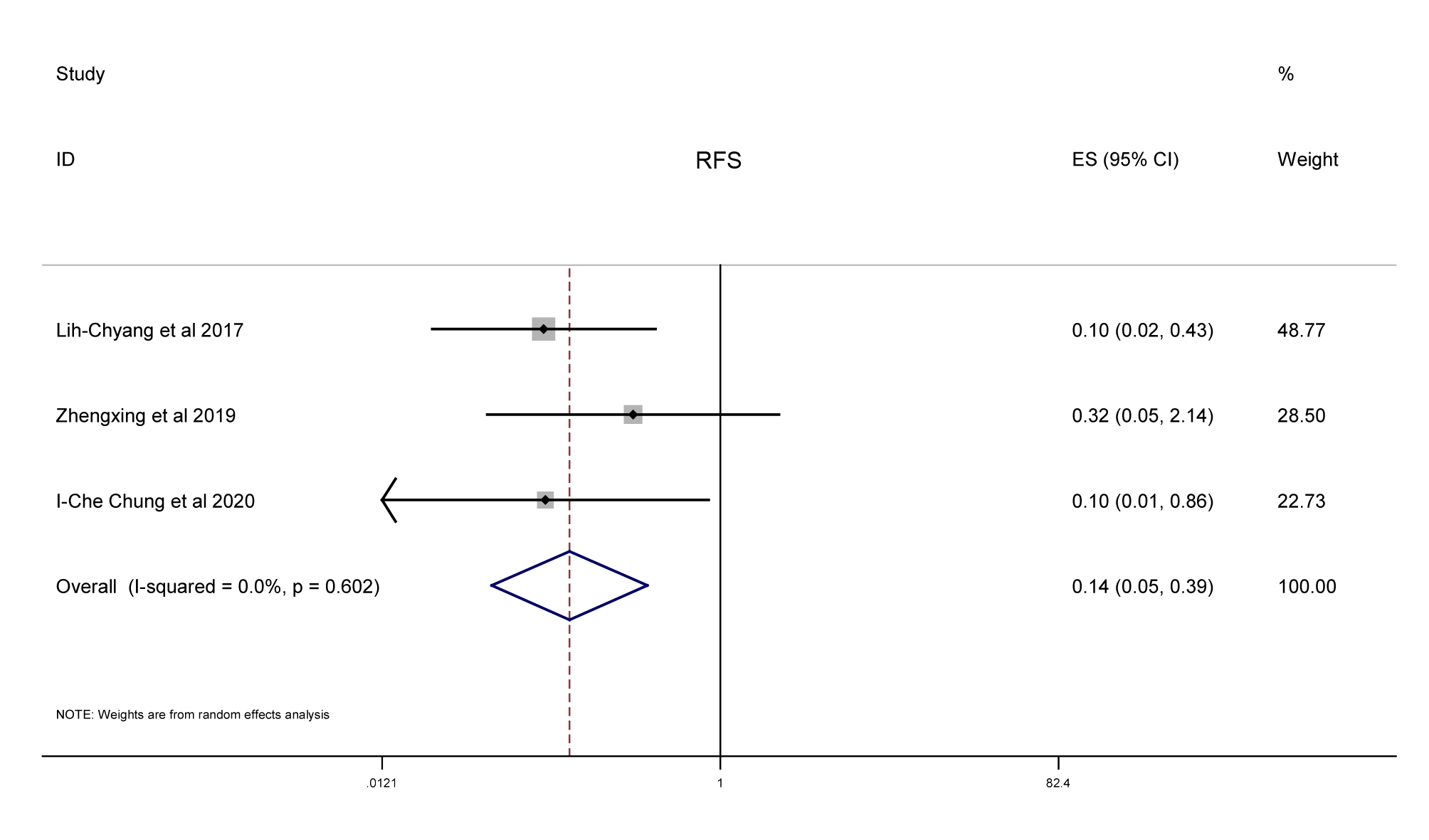
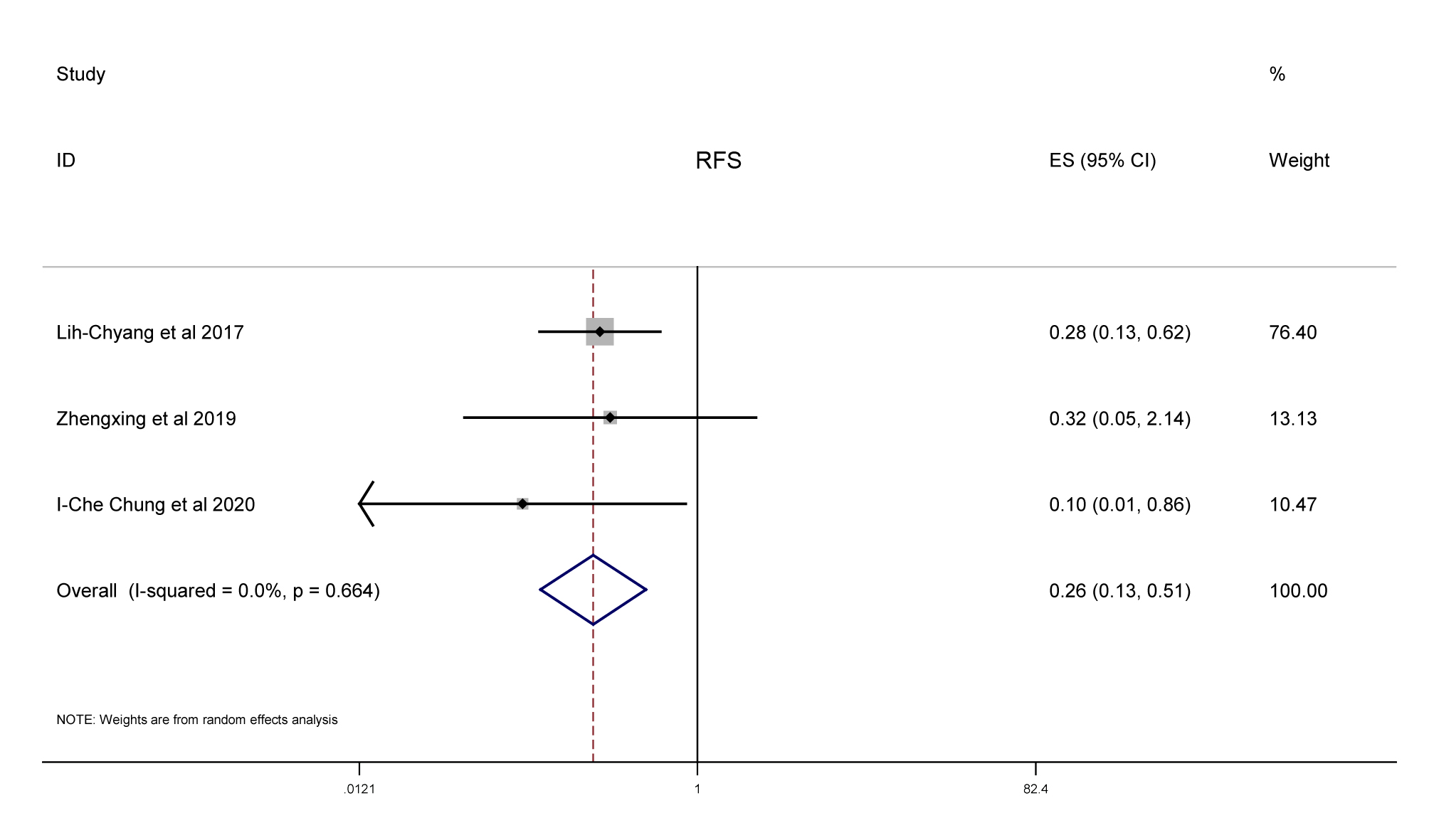
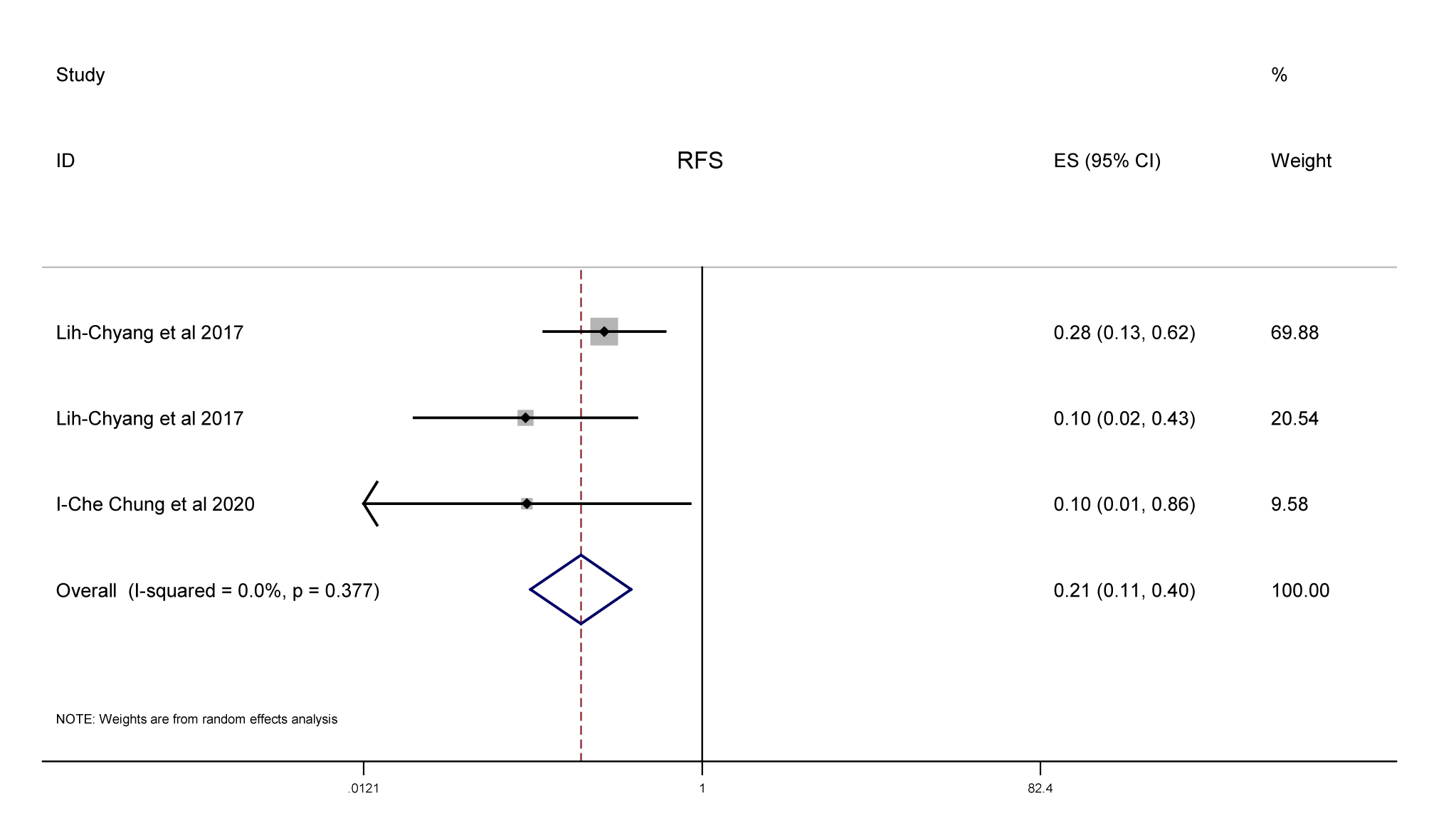
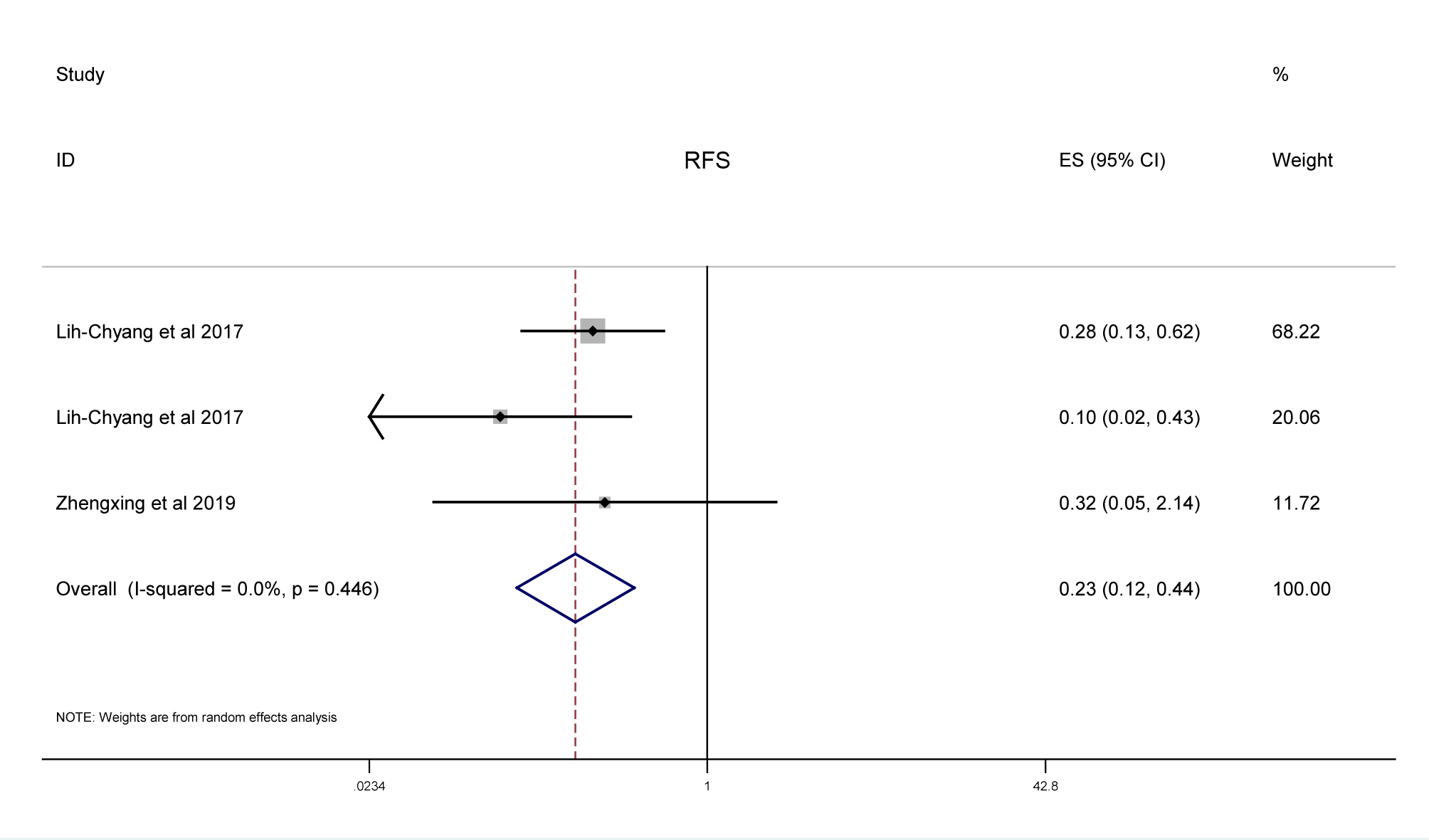
In this study, we conducted a meta-analysis of the available literatures on the roles of inflammasomes in predicting the prognosis of head and neck carcinomas in PubMed, Embase and Web of Science. Then we carried out a meta-analysis of the survival rate, including overall survival (OS), disease-free survival (DFS), and recurrence-free survival (RFS) of head and neck carcinoma patients expressing different levels of inflammasomes.
{kind=link}
{kind=link}
{kind=link}
{kind=link}