Study Design
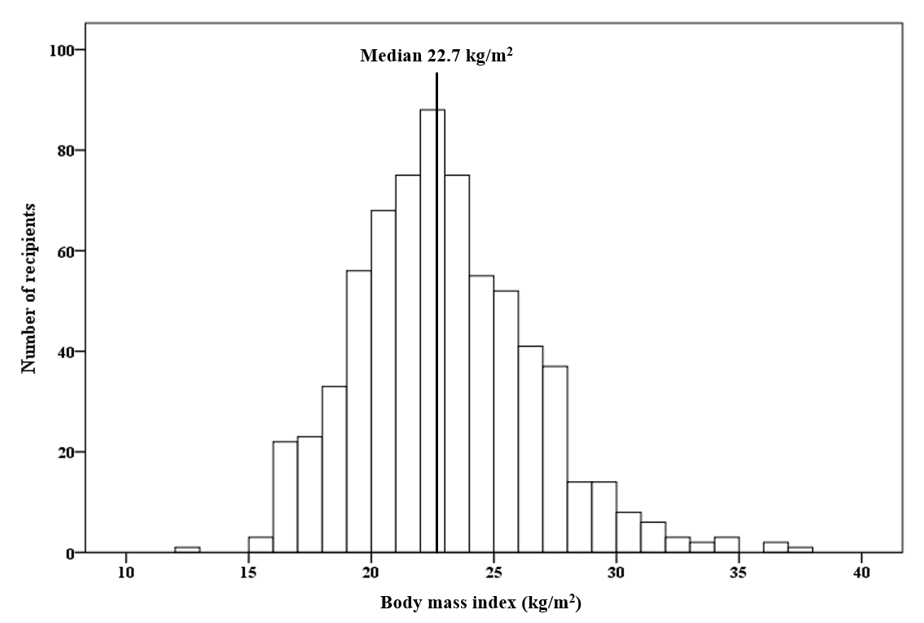
This study was a retrospective, observational and single-center study. Between January 2010 and December 2018, 1290 KTs were performed in Seoul St. Mary’s Hospital. Of these, 412 cases received the kidney from a deceased donor, 195 cases were ABO incompatible KT, and 1 KTR had both legs amputated; these cases were excluded from the study. Finally, 682 KTRs were included in this analysis. The distribution of BMI of the KTRs is presented in Supplemental Figure S1 and the median BMI value was 22.7 kg/m2. Patients with BMI >22.7 kg/m2 were categorized in the high BMI group, while others were classified in the low BMI group. The cases were defined as pre-sensitized to HLA when the MFI value of HLA-DSA at baseline was higher than 3,000 [13] while if the value was below 3,000, they were defined as non-sensitized. Based on the above classifications, KTRs were divided into 4 groups (low BMI-non-sensitized, high BMI-non-sensitized, low BMI-sensitized, high BMI-sensitized) as presented in Figure 1. This study followed the Declaration of Helsinki and was approved by the Institutional Review Board of Seoul St. Mary’s Hospital (XC15RIMI0072K).
HLA Typing, HLA Antibodies, and DSA
HLA typing and HLA antibodies were measured as described previously [14, 15]. Briefly, HLA-A, B, DR, DQB1 typing was performed using the deoxyribonucleic acid molecular typing method using sequence-specific oligonucleotide probes with LIFECODES HLA SSO typing kits (Immucor, Stamford, CT). Lifecodes LSA Class I and Class II kits (Gen-Probe Transplant Diagnostic Inc., Stamford, CT) or LABScreen Single Antigen (One Lambda Inc., A Thermo Fisher Scientific Brand, Canoga Park, CA) were used for detecting HLA antibodies in the recipient sera. According to the manufacturer's instructions, 10 μL of each serum sample was used, and the fluorescence intensities of the samples were measured using a Luminex 200 system (Luminex Corp., Austin, TX).
Desensitization Protocols for Pre-sensitized Patients
The desensitization protocol in our center has been described previously [16-18]. Briefly, the desensitization protocol for HLA pre-sensitized patients consisted of rituximab, total plasma exchange (TPE) and intravenous immunoglobulin (IVIG). Two weeks to one month prior to the transplantation, rituximab was administered, and total plasma exchange using 5% albumin and fresh frozen plasma was performed seven times. The TPE frequency was controlled based on the MFI titer of HLA-DSA. IVIG was administered at a dose of 100 mg/kg over a period of 1 hour after every TPE. In all patients who underwent desensitization, prophylactic agents were used to prevent pneumocystis jirovecii pneumonia (PJP) and cytomegalovirus (CMV) infection. If the crossmatch (XM) test of T-cell complement dependent cytotoxicity (CDC) was positive or HLA-DSA was positive, and the MFI of HLA-DSA did not decrease adequately after 3 cycles of TPE, bortezomib based protocol was used, in which bortezomib was administered for four times in addition to the desensitization protocol.
Clinical Parameters and Outcomes
KTRs’ age, height, weight, history of diabetes mellitus (DM) and hypertension (HTN), cause of end stage renal disease (ESRD), previous dialysis modality, previous dialysis period, and previous KT history were collected as baseline demographic characteristics. In addition, fasting glucose, total cholesterol, triglyceride, high density lipoprotein (HDL)-cholesterol, low density lipoprotein (LDL)-cholesterol, and hemoglobin A1c levels were obtained from the pre-transplant investigations. As a pre-transplant immunoassay, the results of XM test using CDC and flow cytometry-crossmatch (FCXM), HLA-DSA and MFI results by Luminex Single Antigen Assay, and panel reactive antibody (PRA) titers were obtained. Transplantation information was collected for mismatch number, type of induction therapy, main immunosuppressant used, and drug used for desensitization.
We analyzed the incidence of BPAR within 1-year of transplantation (early acute rejection), CMV infection, BK viremia, and PJP rates as short-term clinical outcomes in the 4 groups. The variables used for analyzing long-term clinical outcomes comprised BPAR incidence after 1-year of transplantation (late acute rejection), cAMR, and biopsy-proven calcineurin inhibitor (CNI) toxicity rates. DCGL and patient death rates were also analyzed.
Allograft kidney biopsy findings were interpreted according to Banff classification 2009. BPAR was diagnosed with allograft biopsy as suitable for acute T-cell medicated rejection (TCMR) and acute ABMR criteria according to Banff classification. Similarly, cAMR and biopsy proven CNI toxicity were diagnosed with allograft biopsies according to the Banff classification [19]. Death-censored allograft survival duration was defined as the period from KT to dialysis or preemptive KT, except for patient death in a functioning allograft. Patient survival duration was defined as the period from KT to death due to any cause. Data of changes in allograft function based on serum creatinine levels was collected until 4 years after KT.
The primary outcome of this study was to compare the impact of BMI on DCGL in HLA non- sensitized and sensitized patients. We compared the DCGL rate and death censored allograft survival duration in the 4 groups and analyzed the interaction between high BMI and HLA pre-sensitization status. Secondary outcomes of this study were early acute rejection, CMV infection, BK viremia, PJP, late acute rejection, cAMR, biopsy proven CNI toxicity, patient death rates, and estimated glomerular filtration rate (eGFR) based on Chronic Kidney Disease-Epidemiology Collaboration (CKD-EPI) equation [20].
Statistical Analysis
All continuous variables were expressed as mean ± standard deviation. If the variables followed the normal distribution, an analysis of variance (ANOVA) test was performed. If the variables showed non-normal distribution, a Kruskal-Wallis test was performed. All categorical variables were compared using the chi-square test or Fisher's exact test and expressed as proportions. Multivariate Cox hazard regression model analysis was performed to determine the risk factors affecting DCGL and to investigate the interaction between high BMI and HLA pre-sensitivity. Cumulative survival rates were analyzed during the follow-up period in the 4 groups. Causes of DCGL and patient death were compared using the chi-square test or Fisher’s exact test. The mean eGFR (CKD-EPI) and standard deviation in the 4 groups were evaluated. All statistical analyses were performed using the SPSS® software, version 24 (IBM Corporation, Armonk, NY, USA) and Microsoft Excel 2016.
{kind=link}