Along with the raging pandemic, the world also battled with the dearth of consumables required for testing because of a sharp rise in the worldwide demand. It added to the inadequate hospital care facilities and diagnostic services, delaying the testing further. Pooled-sample testing is a favorable approach under this situation to test a large population or groups quickly with inadequate resources using a highly sensitive RT-PCR technique. Pooled testing is not a new approach, the basic idea was used to test for syphilis (Dorfman et al., 1943). Among others, it has been used in field for various infections including influenza (Van et al.,2012),Chlamydia (Currie et al., 2004), malaria (Taylor et al., 2010) and HIV (Sullivan et al., 2011). Pooled testing could prove to be a favourable approach to take for both, asymptomatic as well as pre-symptomatic cases along with contact tracing and quarantine.
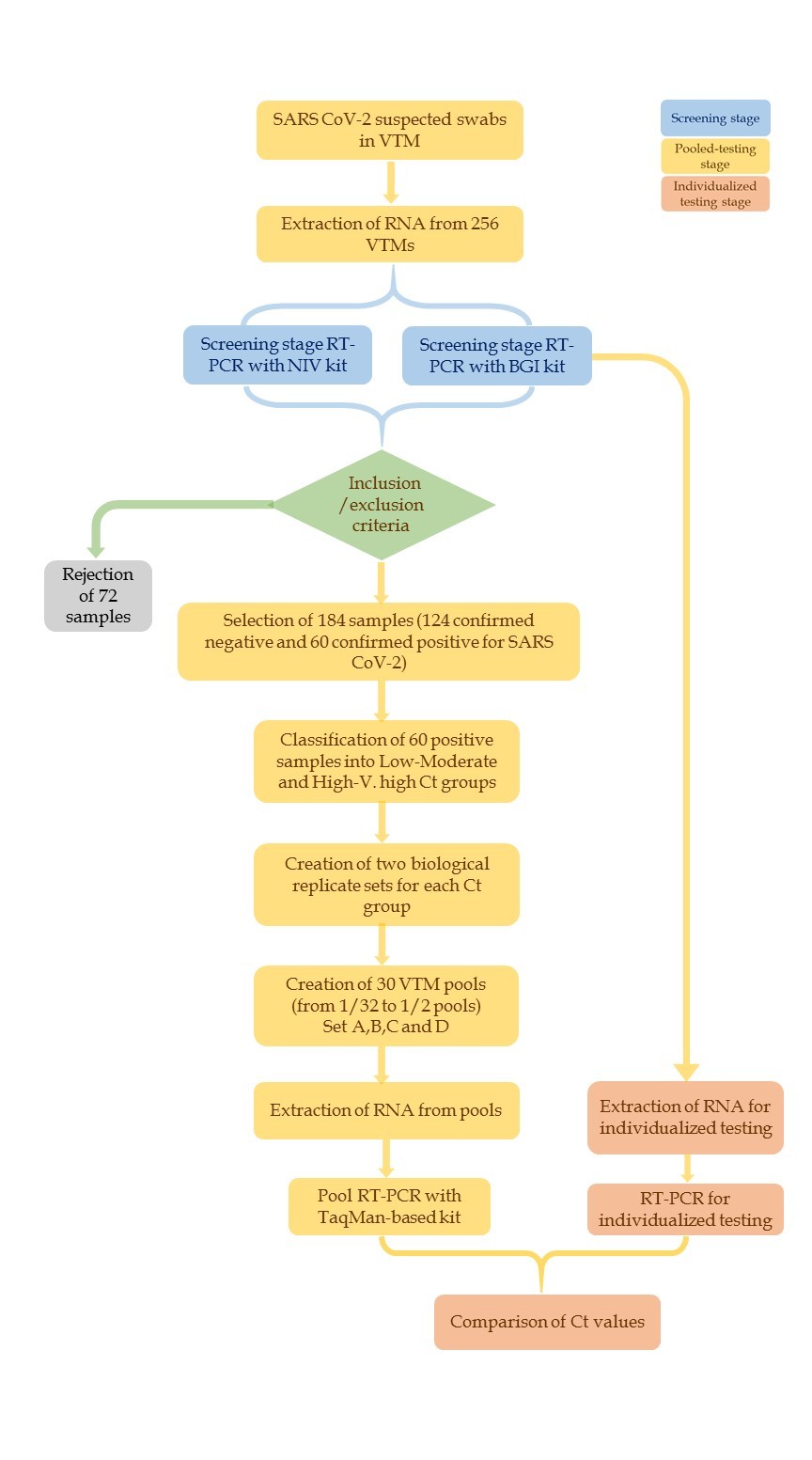
Whenever the question of resource optimization comes especially in the current scenario, one needs to do away with all the steps that increase the cost of the operation. Researchers have attempted pooling using extracted RNA (Gupta et al., 2020; Khodare et al., 2020; Lim et al., 2020), which in our view is not an optimized pooling strategy and does not reduce the resource costs as compared to VTM pooling. This study attempted pooling of VTM samples before RNA extraction, so that repetitive and not to mention expensive exercise of RNA extraction at the initial stages can be avoided all together. This strategy also saves a lot of RT-PCR reactions. This favours the cost-benefit equation of the entire exercise and leads to a substantial reduction in the consumption of consumables, time and manpower- precious resources in a pandemic situation.
One added benefit of the VTM pooling is that it is amenable to different variations of pooled testing strategy e.g. to collect the NP/OP swabs of whole family in the same VTM tube (swab-pooling) and individualized swabs in separate VTM tube at the same time (for sub-grouping stages). VTM pooling and its different variations can also be easily implemented in the door-to-door and Public Health Clinics (PHCs) settings.
This study, presented the data of VTM specimen pooling for detection of SARS-CoV-2 using RT-PCR. Standardization of pooling experiments was performed using samples with a range of Ct values (from low to very high). Our use of samples with different viral load was deliberate to test the pooled testing in different pool sizes. Pooled testing in eight different dilutions, from 1/32 to 1/2 pool sizes was performed. The biological replicate groups used here, checked for between-sample variation. Further, two technical replicates were used to assess the efficiency and reproducibility of the data.Comparison of Ct values between pooled and individual testing was made to determine whether or not the sensitivity of pooled testing is equivalent to that of individual testing.
Some studies (Gupta et al., 2020) have reported better success with pools of lesser number of samples like 2, 4, and 8. Other reports have drawn attention towards the low sensitivity of pooled testing due to the effect of dilution (Theagarajan, 2020). Our results support the observation that larger pool sizes can precisely detect a positive sample without any diminished sensitivity. Based on our results, we believe that a positive sample in even more diluted pools can be detected comfortably (above the 1/32 pools e.g. 1/64 dilution) without any compromise on result sensitivity. As of now few countries (Deckert et al., 2020; Yelin et al., 2020) have demonstrated the regular use of pooling at or beyond a batch of 32 samples to be successful in a low infection positivity rate.
Out of 28 pools (for set A and B) and 32 pools (for set C and D), only one replicate showed absence of amplification (in case of low viral load B32 pool), while its technical replicate gave a borderline Ct of 38.8 (with cut-off being 38 according the manufacturer’s instructions). Although, for the corresponding dilution in biological replicate group (set A), positive amplification was conclusively detected. Any case (except for one discussed above) where borderline Ct would make the diagnostics of pooled samples difficult was not observed. We suggest that this limitation can be overcome by running the RT-PCR for a few additional cycles (this would help especially in low viral load samples). It is also suggested that RT-PCR testing be performed in replicates to increase sensitivity to avoid false negative results and/or performed with 1/28 pooling dilutions as an upper limit.
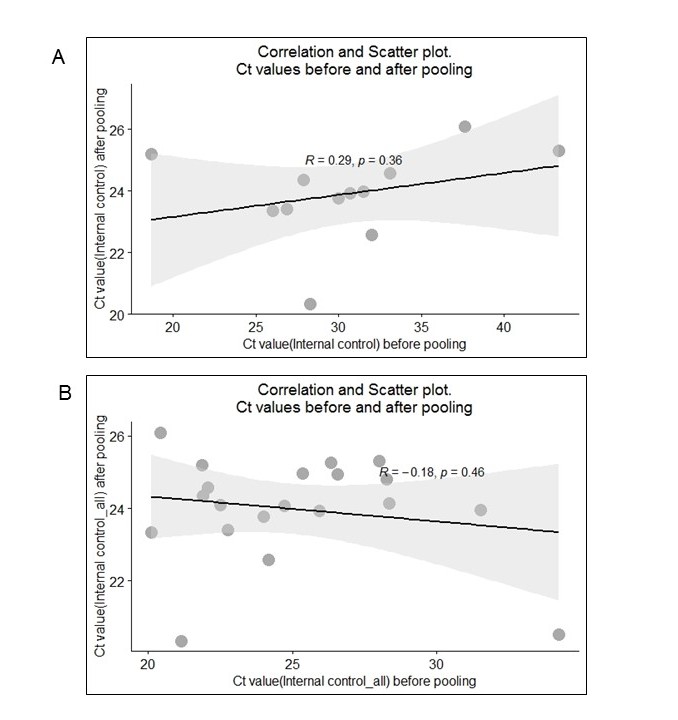
For samples where Ct expectedly increased after pooling, the observed mean Ct value for ORF1ab at individual testing stage was 25.3, while at pooled testing stage it was 27.1, that is, an increase in Ct by 1.75.Despite the increase in the Ct, all the values at pooled testing stage did not give rise to false-negative results and were below the cut-off Ct value (i.e., < 38). On the other hand the mean Ct value for human β–actin internal control for both pooled testing and individual testing stage was observed to be 23.9. It makes sense as the amount of internal control remains constant despite different pooling dilutions.
We observed (Fig. 4) lower Ct values in two retested individual samples. The Ct values were found to be decreased by 0.8 and 1 unit. Other reports have also observed this phenomenon (Lohse et al., 2020). As long as differences are small and occur rarely they could possibly be explained by the random experimental variations during pooling, RNA extraction or PCR stage due to small volumes involved in the PCR. Moreover, both of these cases did not cause the samples being labeled as false-negatives as the Ct values were well below the cut-off range.
The Ct values of internal controls from combined data (from individual testing from 140 µL VTM and pooled testing from 560 µL VTM for all twenty samples from four sets) were also compared. Here also, the absence of any correlation was observed as logically expected (see Additional Figure S2).
One of the strengths of this study is successful implementation of pooling in light of three factors viz. the low amount of input VTM used, the higher pool size tested (up to 1/32) and using samples with low viral. In this study, the lowest amount of VTM used was just 17.5µL in 1/32 pool-size (ranges from 17.5 µL to 35 µL in different pool-sizes) (Table 1). To the best of our knowledge, no other study has reported success in pooled testing with input volume of VTM as low as 17.5 µL in high pool size of 1/32 using low viral load samples (Ct range: 30 to 39). It should be noted that using minimal amount of input VTM allows further saving of reagent costs.
Many studies have attempted pooling but have not reported success when all three variables are considered together (low input VTM, low viral load, high pool-size). This not only makes the present study unique and provides significant improvement over other studies but also emphasizes the scope of widespread use of pooled testing. Many studies have reported false negative results when pooled testing using low viral load samples with relatively higher input VTM volumes e.g. with 30 µL in moderate pool-size of 10 (Ct of ORF1ab: 30.7 to 38.5) (Sahajpal et al., 2020), with 60 µL in pools of 5 and 10, even in triplicates (Lim et al., 2020), with 60 µL VTM in low pool-size of 1/5 (Garg A, Ghoshal U et al., 2020), with 25 to 50 µL of input VTM in pool sizes of 5 and 10 (Garg et al., 2020), with an equivalent amount of 40 µL input VTM in pools of 5 and 10 (Praharaj et al., 2020).
Other studies reported pooling success but with comparatively larger input VTM volume (500/8 = 62.5 µL of input VTM) and low pool-size (1/8) in low-to-moderate Ct samples (~ 17–22, ~ 25–27 and 29-31.8) (Yelin et al., 2020), with 50 µL of input VTM in pools of 5 (Abdalhamid et al., 2020), with 50 to 80 µL of input VTM in low pool sizes of 8 and 5 (Barak et al., 2020).
We also did encounter a failure to detect amplification in one technical replicate at higher dilution of 1/32. Overall we have been able to detect positive sample in higher dilutions in low viral load sample pools in corresponding biological replicate group, especially with such low amount of input VTM. Our results improve upon the set guidelines and highlight the scope of pooled testing for better mass surveillance.
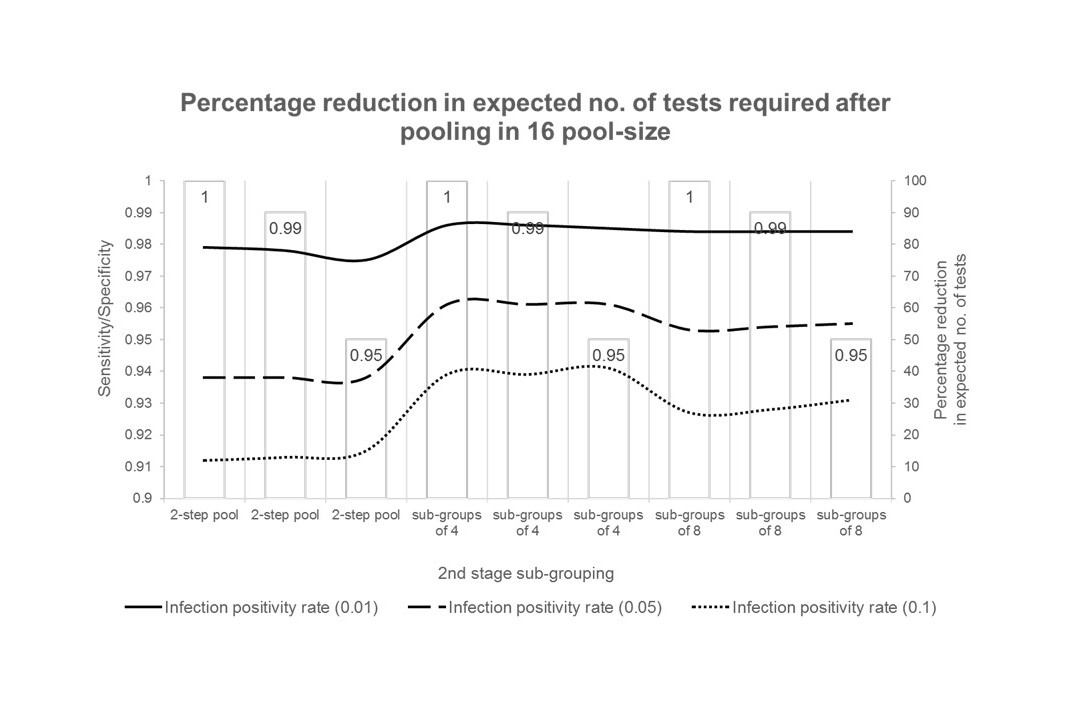
Hierarchical pooled testingis a common pooled testing and sub-grouping method. Using an open-access tool, describing pooled testing and retesting procedures for hierarchical group testing (Black et al., 2015), we looked at the feasibility of the pooled testing approach with respect to different variables. Several variables were considered to calculate their potential in reduction of testing resources. The variables include pool size, sensitivity/specificity of the RT-PCR kit used, stages of pooling, sub-pooling at the 2nd stage pooling and most importantly the test positivity rate (Additional Table 2 and Additional Figure S1).
In view of current pandemic the entire world has been reeling under, the significance of faster diagnostics is of paramount importance. There is an urgent need to screen large groups such as schools, universities, prisons and large workplaces in order to prevent them becoming infection hotspots. Different districts/community pockets and urban-rural settings may show different prevalence. Pooled testing in such eligible settings may lead to early detection of infected people thus help controlling community spread. Since disease prevalence is low now (< 5% in India at the time of communicating this paper), it’s the appropriate time to implement this strategy so that large population/community groups are screened en masse and positive cases isolated immediately to prevent transmission.
Moreover, the real possibility of a new wave caused by mutant strains, including the delta variant (B.1.617.2) and delta-plus variant (B.1.617.2.1/ (AY.1)) is currently making headline along with B.1.617.3 and B.1.1.318 which are already present in India (Cherian et al., 2021). These strains are reported to be more infectious and/or more fatal (Garcia-Beltran et al., 2021; Harvey et al., 2021). These rising mutant strains have started spreading to many countries plausibly due to resuming of international movement – reiterating the importance of pooled testing.
{kind=link}
{kind=link}
{kind=link}