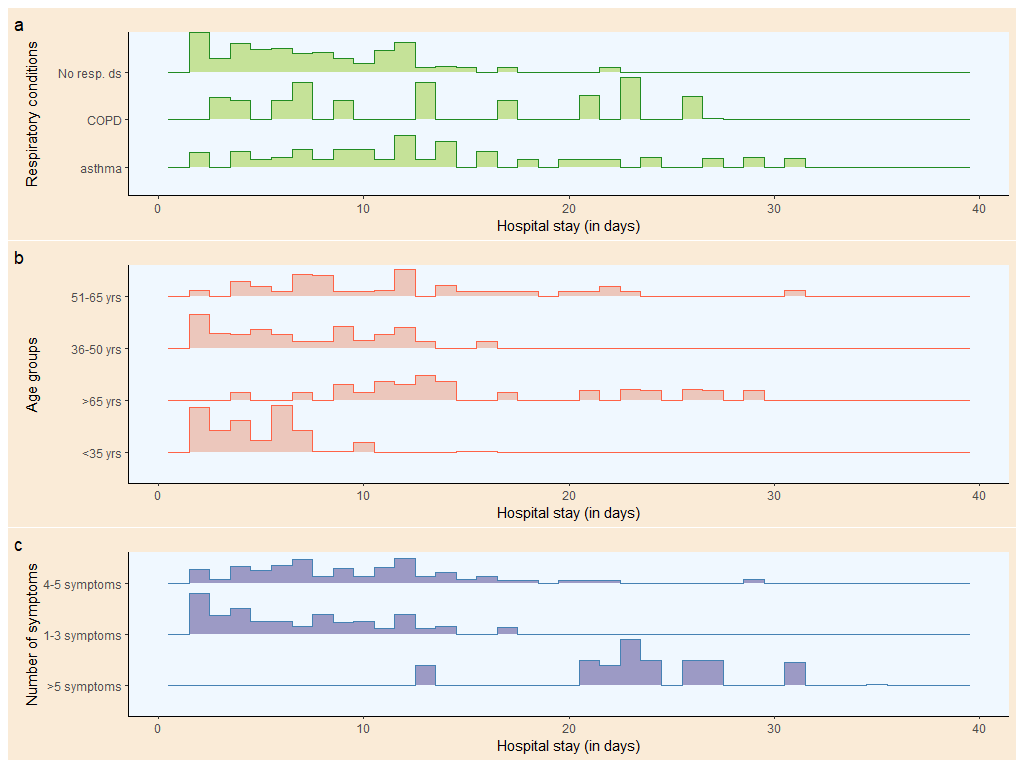
For this retrospective study, we collected data of all the patients admitted to SCB medical college, Cuttack, India, from 25th March 2020 to 31st January 2021. A total of 390,732 patients were admitted to the study site during this period. Out of those patients, 6,918 [4916 (71.06%) male and 2002 (28.94%) female] patients infected with SARS-nCov2 met the study criteria and were included for the analysis. Demographic and clinical parameters have been provided in Table 1. The common comorbidities in the study population (in decreasing order) were diabetes [4127 (59.7%)], hypertension [4031 (58.3%)], and respiratory diseases [3211 (46.4%)]. Before their diagnosis and hospitalization, the common symptoms experienced by the patients before their diagnosis and hospitalization (in decreasing order of frequency) were fever, cough, myalgia, dyspnea, dizziness, anosmia, diarrhea, and hoarseness. The median age of the patients was 52 (39-64) years [male: 53 (40-64) years; female: 50 (37-63) years]. The median duration of hospital stay of patients was 9 (5-13) days [male: 10 (5-14) days; female: 7 (4-12) days] Figure 1(a). Most of the female patients had shorter (< 7 days) duration of hospital stay, and male patients had longer (> 7 days) hospital stay Figure 1(b). There was an increased duration of hospital stay with increased age and number of symptoms. Patients with bronchial asthma or chronic obstructive pulmonary disease were admitted for a longer duration than those without respiratory illnesses Figure 1(c). The duration of hospitalization was prolonged with the presence of respiratory conditions. Supplementary Figure 1 (a) shows that most patients with no respiratory conditions were discharged within ten days of hospitalization. Patients with bronchial asthma had a longer hospital stay in comparison to COPD cases. There was an inclining trend of the duration of hospitalization with the advancing age of the individual, as shown in Supplementary Figure 1 (b). Most patients of age < 35 years had been discharged within ten days of admission. All the patients with > 5 symptoms had to stay for a longer duration (i.e., more than seven days) as compared to those with less symptom complex, as shown in Supplementary Figure 1 (c).
The correlation matrix had been plotted in Figure 2. We found significant correlation of duration of hospital stay with following variables: duration of diabetes (r = 0.78, p < 0.001), age of the person (r = 0.62, p < 0.001), number of symptoms (r = 0.56, p < 0.001), duration of hypertension (r = 0.53, p < 0.001), duration of asthma or COPD (r = 0.52, p < 0.001), and duration of fever prior to hospitalization (r = 0.44, p < 0.001). Other significant correlations were between following variables: duration of dyspnea and number of symptoms (r = 0.58, p < 0.001),duration of diabetes and age of the person (r = 0.55, p < 0.001), duration of dyspnea and duration of diabetes (r = 0.47, p < 0.001), duration of hypertension and age of the person (r = 0.47, p < 0.001), duration of diabetes and number of symptoms (r = 0.45, p < 0.001), duration of asthma and number of symptoms (r = 0.44, p < 0.001), duration of asthma and age of the person (r = 0.43, p < 0.001), and duration of fever and duration of diabetes (r = 0.42, p < 0.001). There was a single negative (non-significant) correlation of duration of hospital stay with duration of alcoholism (r = -0.07, p = 0.921).
For highlighting the associations among age, respiratory illness, number of symptoms, and duration of hospital stay, a Sankey diagram was drawn in Figure 3. The columns (from left to right) represented the person's age, presence/absence of any respiratory disease, number of symptoms experienced before hospitalization, and duration of hospital stay after diagnosis of infection. The widths of the bands denote the association between the variables. Older adults were more affected by asthma or COPD than younger individuals. The patients with COPD had more symptoms than those with asthma and those without any respiratory diseases. The number of symptoms proportionately affects the duration of hospitalization. All individuals with more than five symptoms stayed in the hospital for more than seven days. Most of the patients with asthma & COPD were elderly and were more prone to present 4-5 symptoms at the time of hospitalization, which led them to prolonged hospitalization.
Figure 4 describes the co-occurrence plots of various symptoms of the participants. The up-left plot shows the symptoms in all participants. The up-right portion is meant for the participants hospitalized for 2-7 days. The down-left part depicts the co-occurrence of symptoms for patients hospitalized for more than seven days. The down-right plot shows participants who were hospitalized for more than 14 days. Fever was the most common symptom experienced among the study participants. It mainly co-occurred with cough, myalgia, dyspnea, and dizziness. Here, the size of the circle indicates the percentage of the participants, and the thickness of the line shows the degree of co-occurrence of the symptoms. The co-occurrence plots suggest the direct relationship of the number of symptoms with the hospital stay, which can otherwise be stated as; more the multi co-occurrence of symptoms, the longer is the hospital stay. Our study showed the strongest association with the following symptom complexes: fever - cough (70%) & fever - myalgia (67%). The most petite association was found between loose motions - hoarseness (10%) and dizziness - hoarseness (10%). This finding held good for hospitalization up to 7 days and for > 7 days. But in contrast to the above scenarios, prolonged hospitalization of more than 14 days was strongly associated with multiple symptom complexes, i.e., fever-cough, fever-myalgia, fever-breathlessness, and fever-hoarseness. So fever may be considered as the most crucial symptom associated with other symptoms.
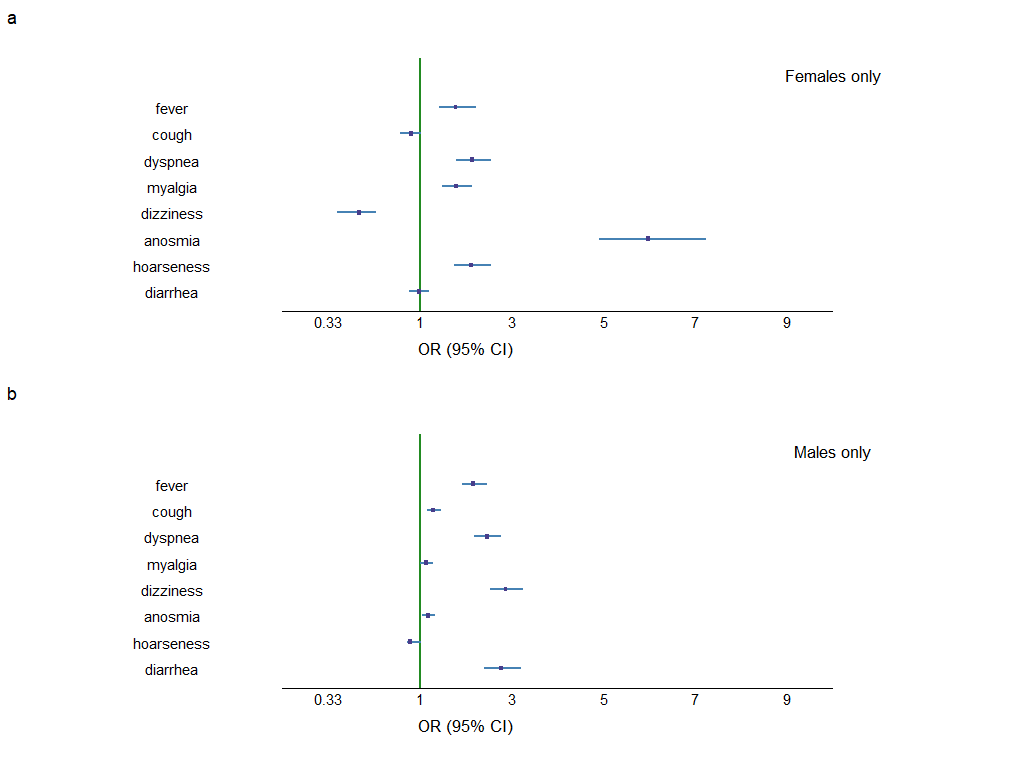
In Figure 5, we analyzed the data to estimate the risk of prolonged hospitalization more than seven days by using the symptoms seen in the patients before the diagnosis of COVID-19. The symptoms (in decreasing order of risk of prolonged hospitalization) were: dyspnea [OR 2.29 (CI 2.07-2.52)], diarrhea [OR 1.98 (CI 1.77-2.21)], fever [OR 1.89 (CI 1.69-2.10)], anosmia [OR 1.86 (CI 1.69-2.05)], dizziness [OR 1.46 (CI 1.32-1.60)], myalgia [OR 1.31 (CI 1.18-1.44)], cough [OR 1.13 (CI 1.02-1.25)], and hoarseness [OR 1.12 (CI 1.00-1.25)]. Subgroup analyses had been done based on gender, shown in Supplementary Figure 2 (a & b). These figures suggested that male patients with symptoms like dizziness, loose motion, dyspnea, and fever were approximately two times more likely to stay for > 7 days in the hospital. And female patients with symptoms like anosmia, hoarseness, dyspnea, and fever were approximately two to five times more likely to stay for > 7 days in the hospital. In contrast to males, females with dizziness were less likely to stay for a prolonged duration.
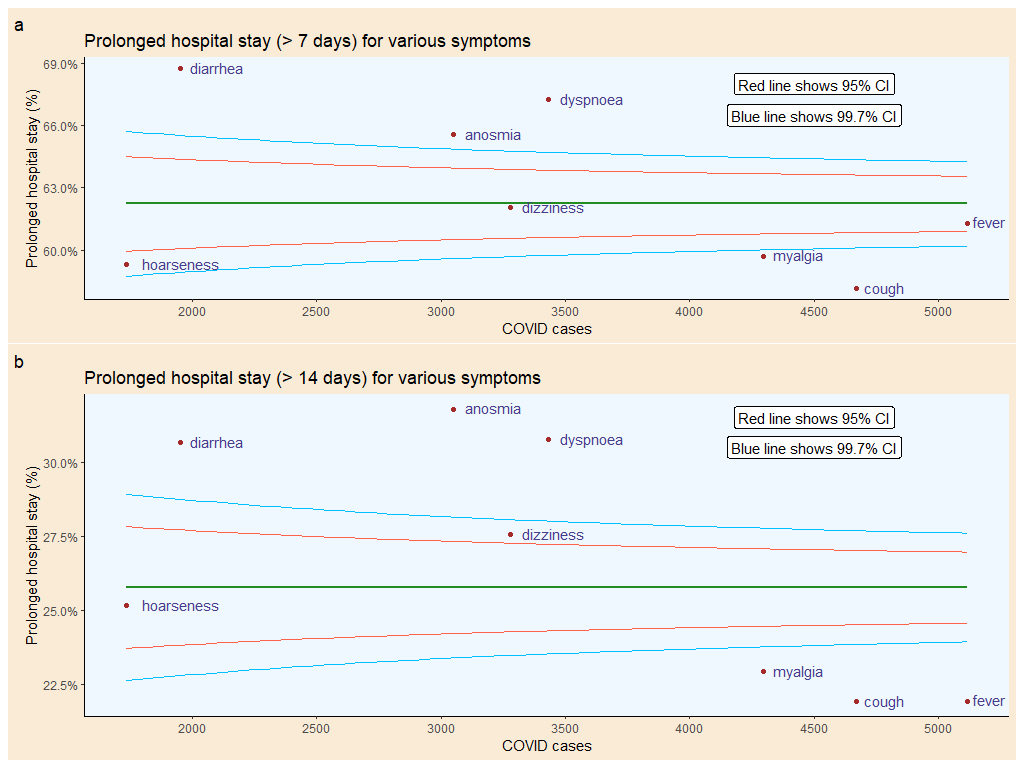
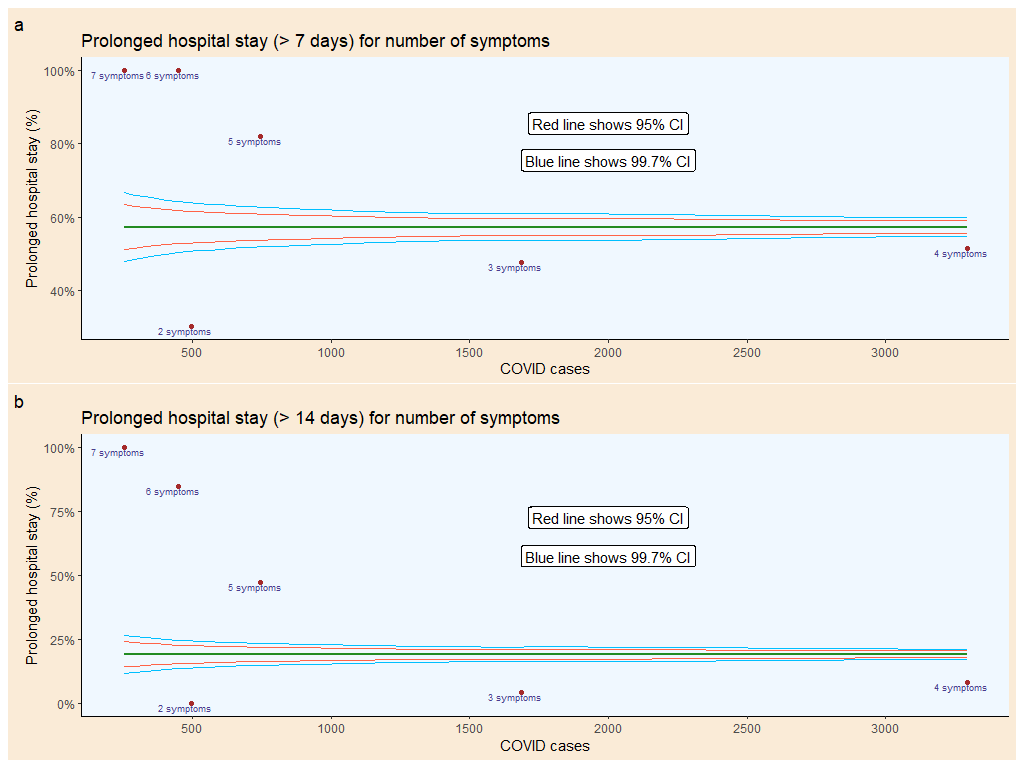
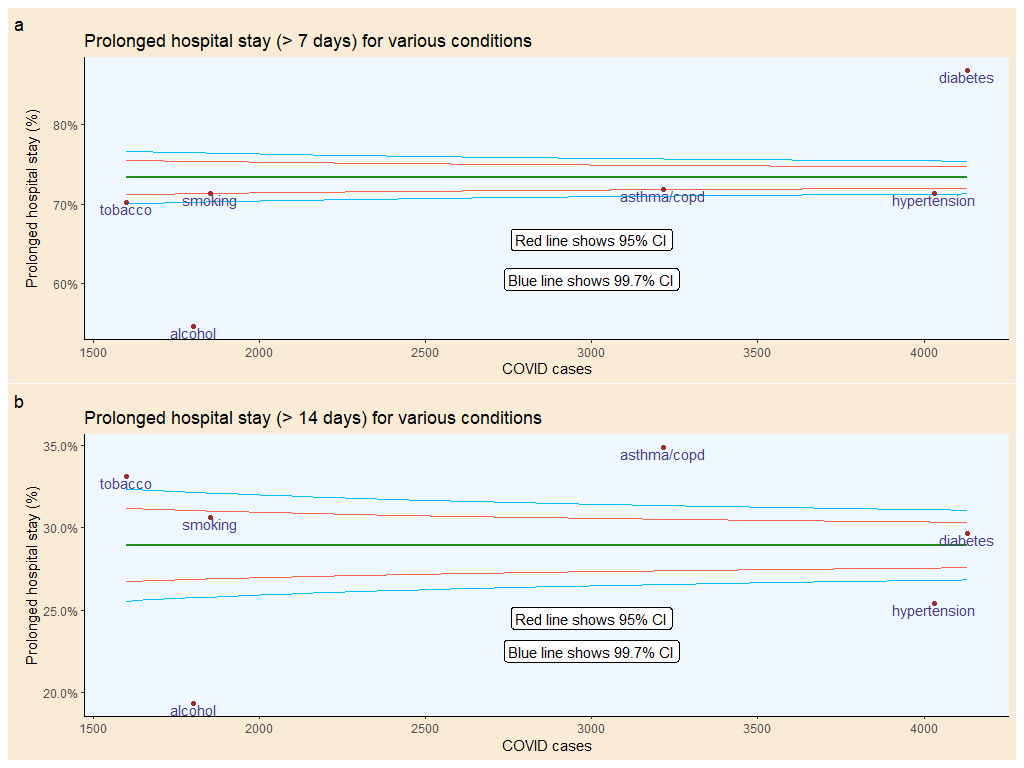
We analyzed the data to find the rate of prolonged hospital stay of the study participants with various symptoms, comorbidities, and addiction(s), and the number of signs and created funnel plots shown in Supplementary Figures 3, 4, and 5. Fever and dizziness are the two prominent symptoms that help predict the rate of hospitalization > 7 days, whereas dizziness and hoarseness are the two critical symptoms that indicate the rate of hospitalization > 14 days. When the numbers of symptoms are taken into account, a combination of 4 symptoms comes close to predict prolonged hospital stay (but outside the CI). Hypertension, asthma/COPD, smoking, and tobacco are the significant predictors for hospitalization > 7 days, but diabetes replaces as a decisive single factor for hospitalization > 14 days.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}