Therapy for SCI remains an ongoing battle in the present era. Limited therapy in SCI is what drives to focus on the therapeutic benefits in the field of SCI. The main obstacle which makes the treatment inadequate is the formation of scar. So far, no medication is available to eradicate the scar formation or restore the neuronal circuit [35]. Even though, Methylprednisolone is approved by FDA for SCI treatment, it is still not considered an ideal therapy due to its severe adverse effect and uncertainty in the risk-benefit ratio [36]. Moreover, the therapeutic drugs used in clinical settings to deal with SCI, remain largely symptomatic therapy. Therefore, these limitations create the need for a therapeutic treatment that can reduce fibrotic scar formation and delineate the neuroprotective effect with minimal side-effects. Herein we studied the effect of ethamsylate, a homeostatic or anti-hemorrhagic drug, widely known for its safe action. It has a multi-faceted mechanism of action, which can be beneficial for its use in SCI. Previous findings suggest that ethamsylate can maintain early hemostasis and thereby improve functional recovery in SCI-induced rodent model [11]. Therefore, we decided to explore the role of the ethamsylate on fibrotic scar formation as well as its effect on mediating secondary damages and exhibiting neuroprotection. So that, it can be repurposed for use in SCI.
In our study, we have administered the ethamsylate intravenously within the 8 hrs of injury, followed by oral treatment for three days. The reason behind opting this treatment strategy is the fact that 8 hours after the traumatic SCI is the most crucial period which determines the long-term effect of the trauma. Therefore, treatment administered within these 8 hrs shows a highly beneficial effect [37]. This is related to the pathophysiology of SCI, in which the primary mechanical damage to the spinal cord causes severe structural damages. In contrast, secondary pathogenesis, which shows cellular damage and tissue destruction, begins within few hours of injury [38]. So, early treatment can reduce the onset of secondary damages. In the long run, these secondary damages lead to the fibrotic scar formation, which acts as a barrier and disrupts the neuronal signal between the two adjacent neurons. This causes the loss of sensory and motor function, as observed in SCI patients. Ethamsylate by virtue of its anti-hemorrhagic and hemostatic effect, decreases the hemorrhagic ischemia in the acute phase of injury, thereby protects the neurons from necrosis and apoptosis. It is well reported that, in SCI, due to mechanical impact, BSCB gets disrupted, which results in the migration of neutrophils and other leukocytes to the injury site [39]. This particular event initiates the cascade of secondary damages. Therefore, maintaining the integrity of BSCB is of foremost importance in SCI. MMP-9, a matrix proteolytic enzyme, is highly upregulated in the acute phase and is involved majorly in the disruption of BSCB via degradation of basal lamina [40]. Thus, it is derived from our findings that ethamsylate preserves the integrity of BSCB as it drastically reduces the expression of MMP-9 as well as increases the expression of TJ proteins such as occludin and claudin-1. Hence, ethamsylate via its ability to decrease the expression of MMP-9 and restoration of TJ protein level protects the BSCB and decreases its permeability. This reduces infiltration of leukocytes and other inflammatory cells to the injury site, thus decreasing the release of cytokines and chemokines at the injury site. Our findings also demonstrated that there was minimal penetration of Evans blue dye into the spinal cord of ethamsylate treated group, which further supports our finding that ethamsylate preserves the integrity of BSCB. After that, we checked the effect of ethamsylate on inflammatory mediators, which initiates the cascade of secondary damages and causes tissue destruction. We noted a significant change in the mRNA expression of IL-1β, IL-6, and TNF-𝛼 between the vehicle and ethamsylate-treated group. So, from this, we can conclude that ethamsylate decreases the release of inflammatory components and reduces the severity of secondary pathogenesis.
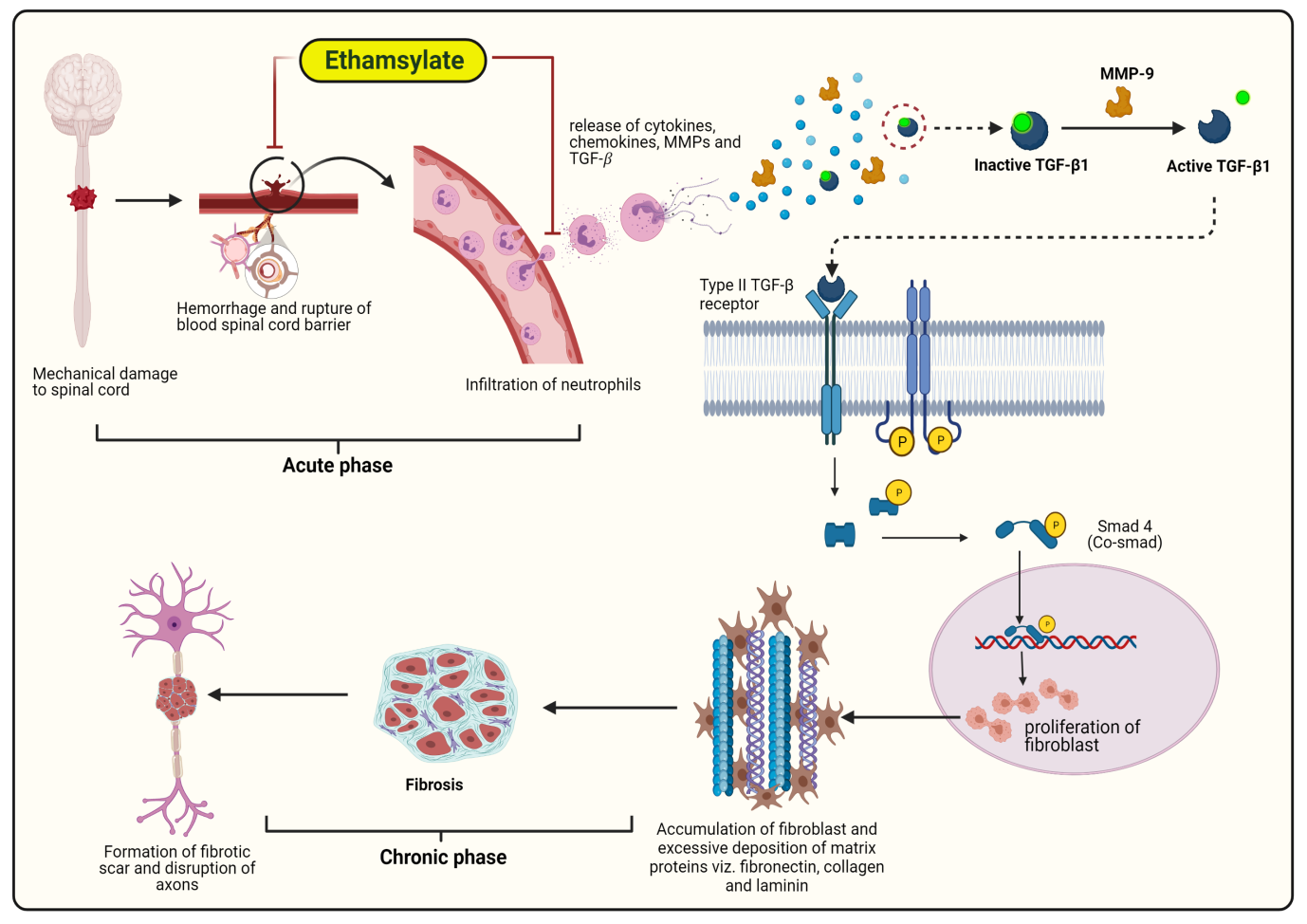
Next, we moved on to the histopathological study of the DPI-28 spinal section using H&E staining. We found a reduced cystic cavity formation at the injured area on treatment with ethamsylate compared to the vehicle group. Moreover, LFB staining of myelin sheath demonstrated increased white matter sparing in the treatment group with respect to the vehicle group. This particularly denotes that ethamsylate reduces myelin degeneration at the lesion area and therefore preserves axonal integrity. These histopathological changes can be correlated with functional recovery observed in the ethamsylate treated group. Besides, behavioral studies data displays a noticeable difference in functional recovery, with the BMS score of the ethamsylate treated group reaching upto 8 at DPI-28 and the vehicle group remained at an average of 3. Then, we further proceeded to look for TGF-β1 level and ECM remodeling at the injury site to determine the extent of fibrotic scar formation. Our immunofluorescence data reveals that TGF-β1, known as the prime suspect behind the fibrosis, is tremendously decreased in the ethamsylate treated group. Moreover, excessive accumulation of fibronectin, collagen-IV, and laminin at the lesion area can be seen in the case of the vehicle group, whereas in the treatment group, the deposition of these extracellular components at the injury site is relatively low. It is reported that MMP-9 predominantly activates TGF-β1 [41], which in physiological condition remains bound with a binding protein, that is in the form of latent TGF-β binding protein (inactive form). MMP-9 cleaves the TGF-β1 from its binding protein, and only activated TGF-β1 binds with type 2 TGF-β receptor and undergoes a downstream signaling cascade which results in excessive proliferation of fibroblast and release of fibronectin, collagen-IV, and laminin, which are the main components of fibrotic scar [8].
As our study depicts that ethamsylate decreases the expression of MMP-9, it directly reduces the activation of TGF-β1, which inhibits the initiation of the fibrotic process and attenuates the fibrotic scar formation. Moreover, TGF-β1 are predominantly secreted by neutrophils and monocytes [42], and migrates to the lesion site due to increased permeability of BSCB after SCI. Ethamsylate stabilizes the BSCB; therefore reduces the production of TGF-β1 at the injured area. Since our findings suggest that ethamsylate can reduce hemorrhagic ischemia, secondary damages, and fibrotic scar formation, it can also be rationalized to exhibit a neuroprotective role. Therefore, we evaluated the expression of NF-H and BDNF in the chronic period. We found that the fluorescence intensity of NF-H and BDNF in the treatment group was relatively high compared to the vehicle-treated group. This uncovers the fact that ethamsylate might also be having a neuroprotective role in SCI. In conclusion, the outcomes of the present study demonstrate that ethamsylate decreases the severity of secondary damages, reduces fibrotic scar formation, and promotes neuroprotection after SCI. Besides, ethamsylate is already a well-established drug in the market with a good safety profile [43]. Therefore, clinical trials of ethamsylate can be performed in SCI patients in the near future as it has the potential to be used in clinical settings for SCI treatment.
{kind=link}