Study setting and data source
The ATTRA registry, established in 2002, is a prospective, national, observational cohort study. Its main purpose is to evaluate the safety and effectiveness of bDMARDs (and lately also tsDMARDs) in patients with chronic inflammatory rheumatic diseases. Patients with RA (and ankylosing spondylitis, psoriatic arthritis, and juvenile idiopathic arthritis) starting bDMARDs or tsDMARDs are recruited from fifty practices sites (private or academic), and captures more than 95% of patients with RA treated with bDMARDs/tsDMARDs in the Czech Republic (CZ). Targeted therapy (TT) has been reimbursed for patients with RA if DAS28 > 5.1 despite therapy with csDMARDs until 2019. Since 2019 the cut-off for DAS28 was lowered to 3.2 in CZ. Initial TT should include either TNF inhibitors (TNFis) or tsDMARDs. At the time of this analysis, the ATTRA database included information on 5050 patients with RA.
At the start of therapy, baseline data are collected including demographics (gender, age at diagnosis, age at the start of 1st line treatment, height, weight, smoking status, presence comorbidities), disease characteristics (disease duration, presence of rheumatoid factor (RF) and anti-citrullinated protein antibodies (ACPA), presence of joint erosions on X-ray), disease activity (swollen and tender joint count (0–28), patient global assessment (PTGA) of disease activity and physician global assessment of disease activity (MDGA) on a 100-mm visual analogue scale (VAS; 0 – best, 100 – worst), erythrocyte sedimentation rate (ESR, mg/h) and C-reactive protein (CRP, mg/L)) and 28-joint disease activity score index (DAS28; 0–10) (18), simplified disease activity index (SDAI, 0–86) (19), Health Assessment Questionnaire (HAQ) for patient function with values from 0 to 3 (the higher, the worse disability) (20), EuroQol EQ-5D questionnaire for quality of life with values from –0.59 to 1 (the higher, the better quality of life) (21), and current or previous anti-rheumatic therapies (csDMARDs, bDMARDs, tsDMARDs) and therapy with glucocorticoids (GCs). Follow-up data on disease activity, disease function and anti-rheumatic therapies are collected after three and six months, and then every six months for three years, with disease activity and anti-rheumatic therapy data collected annually thereafter.
Ethics approval for ATTRA was granted by the Czech Multicentre Research Ethics Committee, no. 201611 S300 and Institutional Ethics Committee of Institute of Rheumatology, Prague, Czech Republic, no. 10113/2016. No additional ethical approval was required for the current analysis. All subjects provided their written consent for the collection and storage of data before participation. All procedures were performed following the Declaration of Helsinki.
Study population
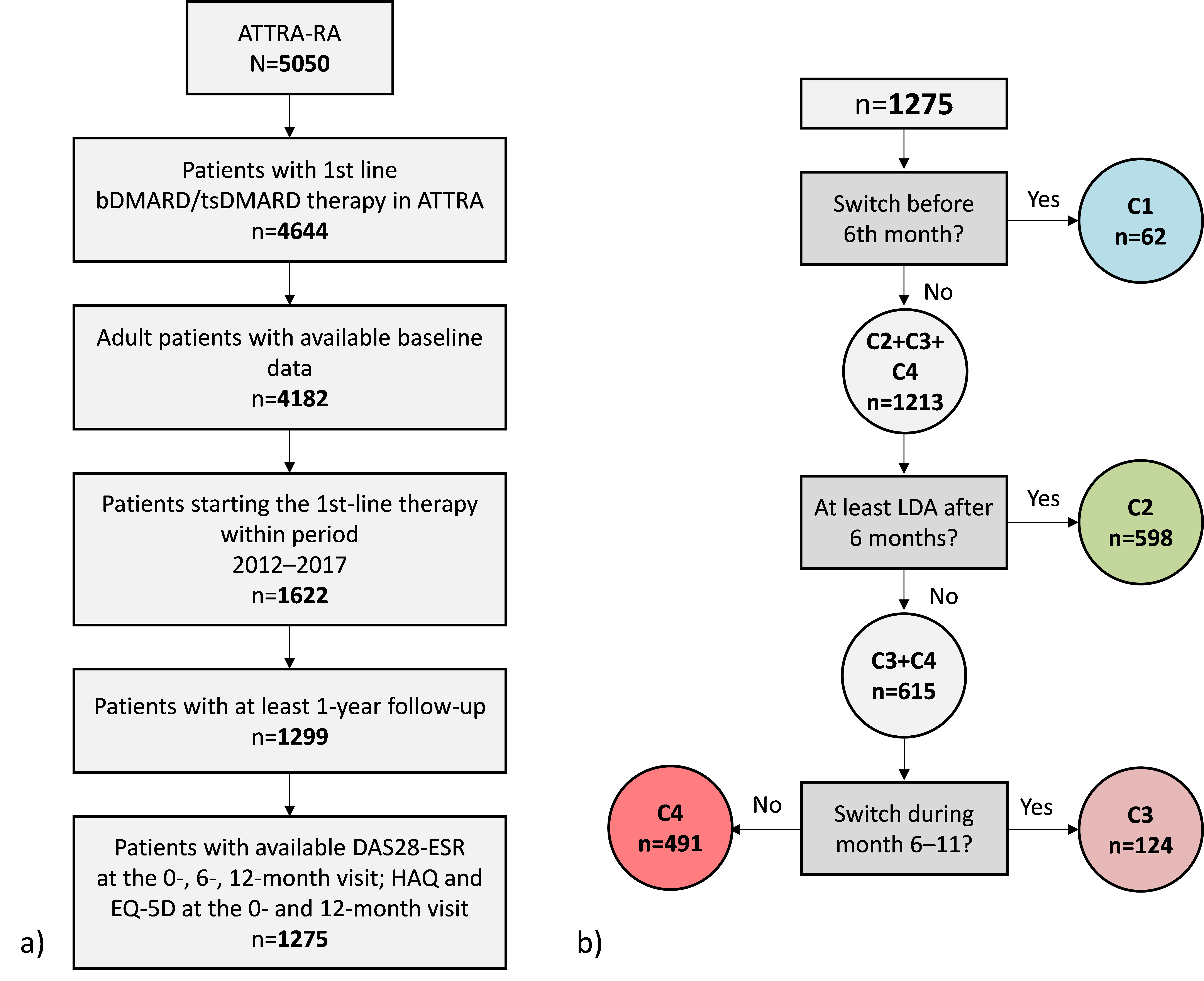
In this study, we included all bio-naive adult patients diagnosed with RA starting bDMARDs/tsDMARDs within a period from 1 January 2012 to 31 January 2017 with at least one-year follow-up. Patients without available DAS28-ESR at baseline, 6-month and 12-month visit or without HAQ and EQ-5D at baseline and 12-month visit were excluded (see Supplementary Figure 1).
Study design
We divided patients into four cohorts based on a treatment result at the 6-month visit and based on switches to another therapy during the first year of the treatment (Figure 1). First, we evaluated whether patients switched to another therapy within the first five months of the treatment. Next, we assessed if patients reached remission or low disease activity at the 6-month visit (defined as DAS28‑ESR ≤ 3.2). Finally, we checked whether patients changed the therapy within months 6–11 provided they did not achieve the treatment target. Cohort C1 includes patients that changed bDMARD/tsDMARD therapy during the first months (usually at 3-month visit) before evaluating treatment response at the 6‑month visit. These patients were either not responding to the treatment at all, or were not tolerating the treatment (e.g., side effects) within the first months of the first-line therapy. Cohort C2 consists of patients ideally responding to the treatment because they achieved the treatment target after six months of therapy without a need to switch. Cohort C3 comprises the group of patients not responding to the treatment, because they did not achieve the treatment target after the first six months of therapy. Following T2T principles, they switched to a different treatment. The last cohort C4 is represented by patients not responding to the treatment since they did not achieve the treatment target (similarly to C3 cohort). Regardless of T2T principles, they continued with the same treatment.
Objectives and Outcome measures
The primary objective of this study was to compare odds for the achievement of REM or at least LDA after one year of the treatment between patients following and not following T2T strategy (C3 vs C4). We assessed disease activity DAS28-ESR index; specifically, LDA was defined as DAS28-ESR ≤ 3.2 and REM was defined as DAS28-ESR < 2.6. In terms of the secondary outcomes, we compared treatment results based on DAS28-ESR after 12 months between all studied cohorts. The proportion of patients with remission (REM; DAS28‑ESR < 2.6), low disease activity (LDA; 2.6 ≤ DAS28-ESR ≤ 3.2), medium disease activity (MDA; 3.2 < DAS28-ESR ≤ 5.1) and high disease activity (HDA; DAS28-ESR > 5.1) at baseline and 12-month visit were compared across the studied cohorts C1–C4. Next, we compared changes in parameters related to disease activity (DAS28‑ESR, SDAI, tender and swollen joint count, CRP, ESR, PTGA, MDGA) and quality of life (HAQ-DI, EQ-5D) after 6 and 12 months of the bDMARDs/tsDMARDs treatment between cohorts C3 and C4.
Statistical methods
Descriptive summary of patients’ demographic and treatment characteristics and disease activity measurements was performed for all four studied cohorts C1–C4. For continuous variables, we calculated the median with interquartile range (IQR, 25th–75th percentiles). For a description of categorical variables, we used absolute and relative frequencies (i.e., percentages). To test differences between two patients’ groups, we performed the non-parametric Mann-Whitney U test for continuous variables and Pearson’s chi-squared test for categorical variables. The magnitude of changes in parameters over two visits was tested through the paired Wilcoxon test. For all tests, P‑values < 0.05 were considered to be statistically significant. We did not impute missing data in this analysis and performed a complete-case analysis instead. The percentage of missing data in outcome variables (i.e. DAS28-ESR, HAQ and EQ-5D at baseline, 6 and 12 months) was relatively small; we excluded 1.8% of patients in total.
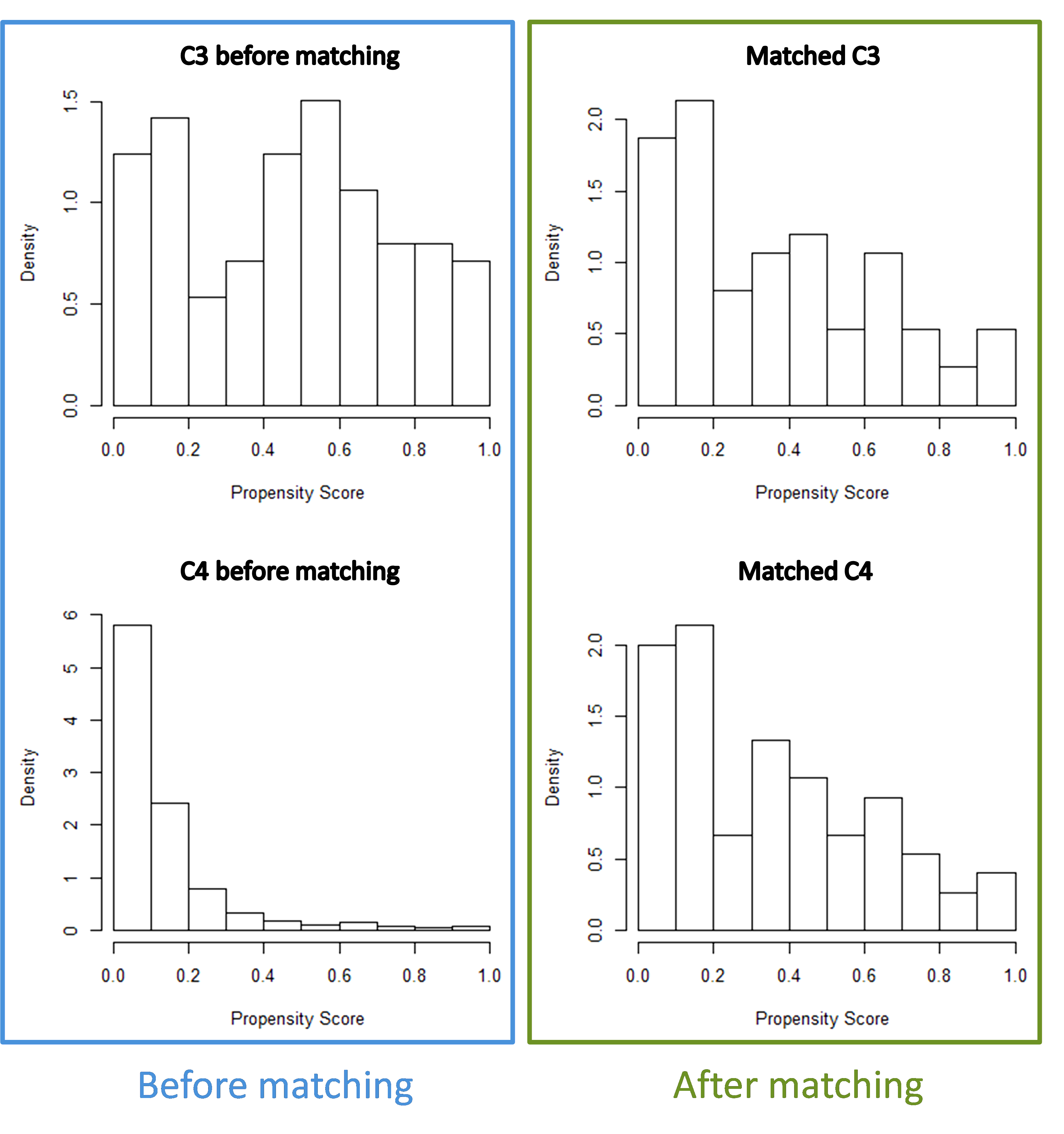
We used propensity score matching to match patients not switching to another therapy after not reaching treatment target at 6-month visit (C4) to patients switching to a different treatment after not reaching treatment target (C3). For matching, we performed logistic regression with outcome variable C3 (=1) vs C4 (=0) and covariates: gender, age at the start of 1st line therapy, disease duration, number of previous csDMARDs, glucocorticoids in previous therapy, swollen joint count, tender joint count, PTGA, ESR, CRP, HAQ, RF positivity, presence of comorbidities, smoking, csDMARDs in concomitant therapy and glucocorticoids in previous therapy. We chose the matching ratio 1:1 and set the caliper to a value 0.2. We used matching to make both groups comparable in characteristics at 6-month visit and to minimise confounding by other factors in the evaluation of achieving REM/LDA at the 12-month visit. After we carried out propensity score matching, we employed binary logistic regression to determine the odds for reaching of REM/LDA at the 12-month visit in cohort C3 and C4. We did all descriptive statistics and testing using IBM SPSS Statistics 25.0. Propensity score model was performed in R (version 3.5.3).
{kind=link}
{kind=link}