Data description and screening
Epidemiology and demographics
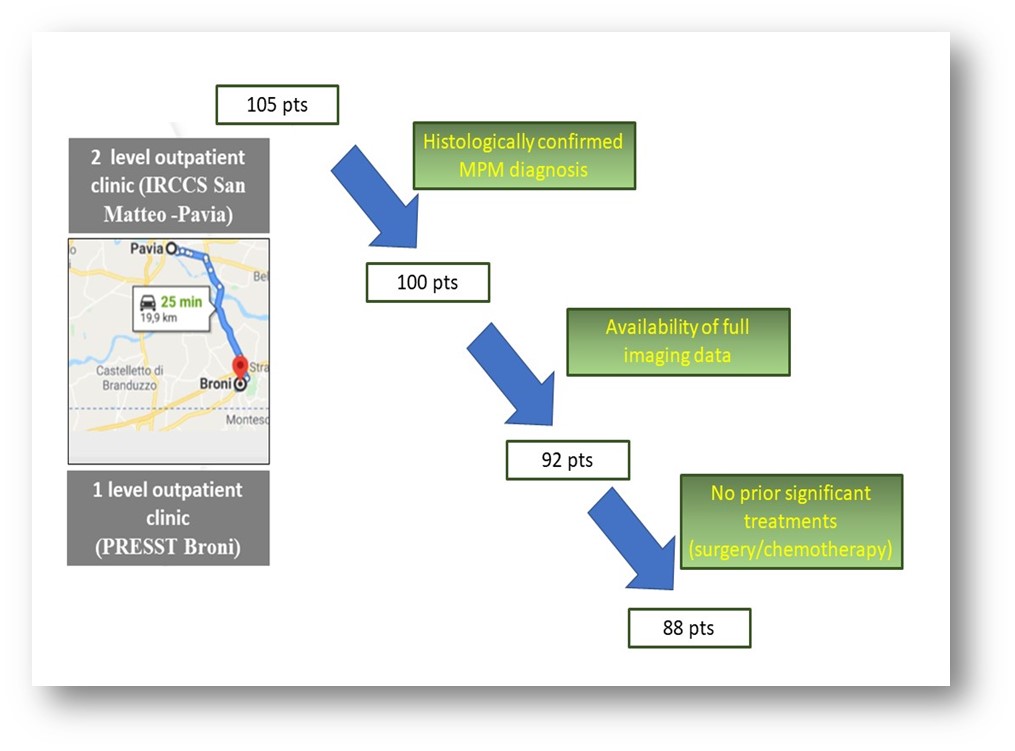
The total number of patients referred to our Territorial Diagnostic, Therapeutic and Assistance Planning was 105. From there, 17 patients did not fit our inclusion criteria. In our raw data, we looked at more than 30 parameters in 88 MPM patients between November 2018 and May 2020. Patients enrolled in clinical trials were excluded from the analysis. Exhaustive clinical data are summarized in Table 1. Of them, 26 (29.5%) were females and 62 (70.5%) were males. The male-to-female ratio we report is roughly 2.3, which is near that reported in the 6th edition of the ReNaM report (M:F = 2.5) [6]. The male predominance was expected as exposure to asbestos often occurred in and around industrial factories where most employees were men. The average age at diagnosis supports this concept: it was of 68.9 years (from 47 to 85 years), with a median age of 71. This data is broadly in line with that of the 6th ReNaM report, which shows an average age at diagnosis of 70 years [6]. No cases of diagnosis under the age of 47 were found in our study, confirming what is contained in the ReNaM report where only 2% of total cases recorded occurred in patients younger than 45 years and coherently to the significant latency associated with the disease onset after exposure to asbestos. The majority of the patients observed had a significant exposure to asbestos as part of their employment/family/social history. Indeed, 24 out of the 88 patients reported certain or highly probable workplace exposure (either directly from the factory or indirectly through various blue-collar work). Environmental and indirect exposure (patients were relatives of workers in asbestos industrial plants) cases were significantly higher (30 cases, 34%) as the pollution from the factories had an effect on members of the town. The significant environmental pollution and massive exposure during the company's peak activity period (1970s and 1980s) created this high incidence, as previously mentioned. No relevant exposure history was reported for 30 (34 %) of the patients in our cohort. Out of the 88 total patients, 36 (40%) claimed to have never smoked, while 15 (17 %) were active smokers and 37 (42 %) were ex-smokers. Thus, 59% of the analyzed population referred a smoking history coherently to previous studies showing important synergistic tumorigenic activity of smoke and asbestos, related in both cases to induction of inflammation and directly damaging DNA [13,14]. Indeed, even with equal asbestos exposure, cigarette smoke has been correlated with increased risk of developing MPM [15].
Radiological and clinical diagnosis and staging algorithms
Of all 88 patients followed, we aimed at identifying key radiological features at baseline (Table 1). However, a history of thoracentesis or drain placement was permitted, as this would not alter plaque/tumor size. Despite the fact that most of our patients had a significant pleural effusion, most had not received thoracentesis or drainage before the “indicative” or “diagnostic” CT scan was taken. Indeed, just 14 patients (16%) had evidence of a previous evacuation of pleural fluid via drain or thoracentesis on radiologic reports or CT images. On the other hand, only 4.5% (4 cases) of patients had no pleural effusion. Four patients had evidence of bilateral pleural effusion on pre-treatment CT scans. Thus, the 96% pleural effusion prevalence reported in the population of study was higher than already published data [16,17] among which the 79% found by Dogan et al. in a CT analysis of 212 patients with MPM in Turkey [18] although some different features in terms of patient population, time-period analyzed, environmental and epidemiological factors define the two cohorts. In our study, 34 (39%) patients showed bilateral alterations (pleural effusion, pleural plaques or chest wall infiltration) whereas 64 (73%) showed mediastinal involvement at time of diagnosis. Roughly half of our patients (45 patients or 51%) had some sort of involvement of the diaphragm before receiving chemotherapeutic treatment.
MPM diagnosis confirmation has been reached through three main approaches, namely medical thoracoscopic, percutaneous and surgical biopsy (Table 1). Of them, medical thoracoscopy was the most common (50 patients or 56.8 %). Percutaneous biopsies and surgical procedures (VATS) were used in 19 patients (21,5 %) respectively, while no patient received diagnosis through cytology on pleural fluid. Biopsy results showed that most of our patients received a diagnosis of epithelioid-type MPM (66 patients or 75 %). This result is in-line with the reports from AIOM 2018 guidelines that showed a prevalence of the epithelioid histotype in 75-80% of cases [website at https://www.aiom.it/wp-content/uploads/2019/10/2019_LG_AIOM_Mesotelioma.pdf], but is significantly higher than the percentage of epithelioid cases reported in the ReNaM (55% of cases) [6]. Coherently to already reported data, the epithelioid histotype was associated with an increased overall survival (15.72 months vs 13.2 months in sarcomatoid cases and 11.8 in biphasic ones). The diagnosis of a sarcomatous/desmoplastic lesion was found in 6 patients (6,8 %) and the biphasic type in 7 patients (7,9%) respectively, being less represented than the data reported in ReNaM, where the biphasic histotype accounts for 10.5% of cases [6]. These percentages are also slightly different from those reported in the AIOM guidelines, where the biphasic histotype is attested to 10-25% of cases and the sarcomatoid about 10%. In nine patients (10.22%) it was not possible to define a precise histotype even in the presence of certain MPM (defined as unspecified mesothelioma). This data is broadly in line with the ReNaM, where 12% of MPM are not otherwise specified (NOS).
Of the 88 patients observed, 23 were stage IA, 14 patients were stage IB, 30 patients were stage II, 5 patients were classified as IIIA and 9 as stage IIIB. Finally, seven patients were classified as stage IV, indicating that distant metastasis was found (Table 1). Overall, the 76% of patients have an early stage of disease (IA-B, II) according to the TNM-8 Ed system [19]. As a result, the majority of patients were susceptible to surgical therapy and/or multimodal approach.
Treatments
More than half of the 88 patients in our study received some form of surgery as a treatment for MPM (52 patients or 59,1%). Of these 46 patients received pleurectomy/decortication surgery. Six patients received various other palliative surgical approaches. These data correlate with the fact that most of the evaluated patients had low-stage tumors (TNM stage I or II), thus eligible to surgery. In all cases, P/D was followed by conventional chemotherapy and 21 patients had a progression free survival higher than 10 months. Chemotherapy was the most common therapeutic option and 67 out of the 88 patients received the standard first line chemotherapy regimen made of pemetrexed and cisplatin; 18 patients underwent mono-chemotherapy (carboplatin) due to the low performance status and comorbidities. The timing of the treatment was not the same for all patients though: 4 (6%) of the 67 patients received neoadjuvant treatment and remaining underwent adjuvant chemotherapy. Side effects of the chemotherapy were not specifically monitored, but we did not report severe toxicities. Second line treatments were performed in 52 patients: 30 of them were treated with gemcitabine, 19 with vinorelbine and three underwent first line chemotherapy re-challenge.
Out of the 88 patients we followed, just 7 patients (8 %) received radiotherapy (RT). In three cases RT was a part of multimodal treatment, while 4 patients received radiotherapy for palliation.
Data are detailed in Table 1.
Outcome
The number of months that a patient was “disease-free” was reported for all and the range was extremely heterogeneous between 3 and 45 months with an average value of 9,8 months. The average time to progression after second line chemotherapy was 4.6 months. The overall average survival (OS) was 15.6 months irrespective of tumor histotype whereas higher values are observed in female patients (mean 18.23 months vs 14.55 months in women and men, respectively)
Statistical analysis and data mining
We then moved to analyze the records through partition analysis to explore combination of factors that impact essentially on clinical outcome to identify and select and the most relevant predictive and prognostic variables. Differences emerged by subdividing the cohort based on patient gender. We thus focused on the most relevant outcome parameter, namely overall. We expected that the high number of early stage diseases in the population in study would correlate with a relatively better prognosis if compared to advanced ones, but, quite surprisingly, no statistically significant association could be identified between OS and TNM stage at diagnosis (Fig.1, panel I). The most relevant variable associated to OS in women was determined by access to second line treatment since those patients who did not underwent to it displayed a significantly lower OS (12.5 months vs 22.4 months). Among patients who received second line therapy, the subsequent split underlined that exposure to cigarette smoke (past and /or current) significantly affected mortality (average OS 18.7 months). Although, performance status (PS) should be a limitation in defining therapeutic strategies, these data suggested that at least in in never smoker female patients, comprehensive chemotherapeutic regimens can assure better outcomes (mean OS 25.6 months). Within respect to male patients, it should be noted that no significant splits could be found when patients were stratified by age. When removing this variable from the analysis, chemotherapy schedule significantly impacted on OS and treatment with platinum and pemetrexed was associated to OS rates (15.4 months) higher than platinum alone (11.4 months). Coherently, concomitant advanced disease stage was associated to worse prognosis (mean OS 5 months). Again, although PS and comorbidities might drive decision on treatment schedules, these findings confirmed that doublets should be the preferable conventional chemotherapeutic regimen. Results are available in Fig1, panel II. It should be noted that these findings impacted on long term overall outcome and no significant differences can be found by evaluating chemotherapy regimen and progression free survival in both men and female patients (Fig.1, panel III). Since no clear data are available in literature on the most beneficial conventional chemotherapy agent [20,21], we proceeded to analyze data regarding II line treatments. Specifically, we compared the efficacy of gemcitabine (30 patients) vs vinorelbine (19 patients). We excluded from the analysis the three patients who underwent first line chemotherapy re-challenge. Within the limit of the cohort analyzed, vinorelbine emerged as the most advantageous choice but only in female patients whereas in male subgroup the Student’t test comparing the pair did not reach a statistical significance (Fig1, panel IV).
{kind=link}