Patient selection
This retrospective review of prospectively collected data included the review of all 336 patients who underwent PD for periampullary lesions between January 1, 2008 and March 31, 2020 in the study institution. The institutional review board approved the study protocol (approval number: HM19-064).
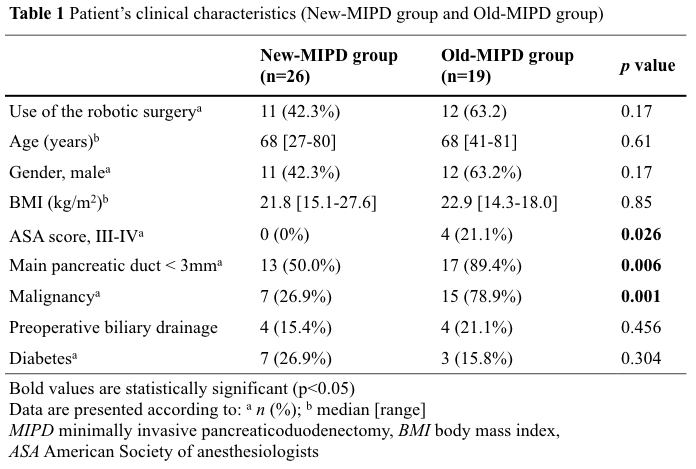
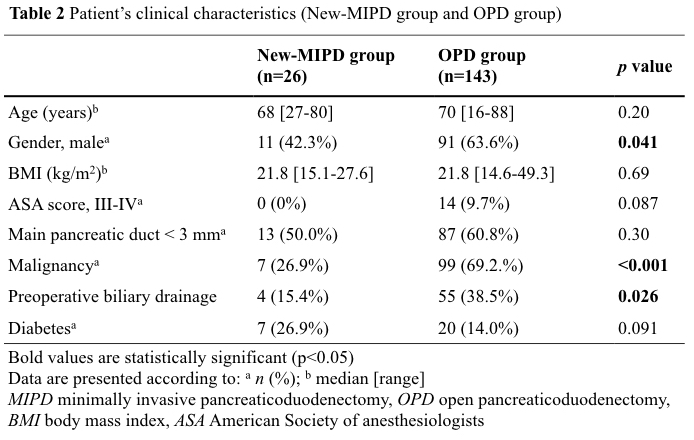
The present study included 188 patients with a soft pancreatic texture among the 336 patients. First, the degree of pancreatic fibrosis in pancreatic remnant was subjectively classified as soft or hard by experienced pancreatic surgeons during surgery and 146 patients with a hard pancreatic texture, including 35 patients who required concomitant resection and reconstruction of the vasculature and/or other organs, were excluded. Two patients who underwent PJ via a small upper middle incision by conversion from MIPD were also excluded from the study cohort. The remaining 188 patients who were included in the final analyses were classified as follows: OPD group, 143 patients who underwent OPD with conventional PJ between January 2008 and March 2020; Old-MIPD group, 19 patients who underwent MIPD with conventional PJ, including seven patients who underwent LPD between 2008 and 2016 and 12 patients who underwent RPD between 2009 and 2016; New-MIPD group, 26 patients who underwent MIPD with the Kiguchi method between September 2016 and March 2020, including 15 patients who underwent LPD and 11 patients who underwent RPD. In the RPD group, the da Vinci Si or Xi platform (Intuitive Surgical, Mountain View, CA, USA) was used. The patients enrolled in the study are summarized in Fig. 1.
Development of the Kiguchi method
Based on our experience, the high POPF rate in MIPD using conventional PJ is attributed to several technical errors even with robotic surgery. Briefly, these potential technical errors are primarily a result of the motion restriction of forceps, insufficient water tightness of the PJ, and entanglement and confusion of the many threads. The Kiguchi method is a simple and feasible PJ technique to resolve these technical errors which are intricately intertwined with each other.
Details of the Kiguchi method
Patient position and placement of trocars
The patient is placed in a reverse Trendelenburg position. In LPD, five trocars, including three 12-mm and two 5-mm trocars, are used for resection and two 3-mm trocars are added for PJ (Fig. 2). In RPD, five trocars, including one 12-mm and four 8-mm trocars, are used for resection and one 12-mm trocar is added for PJ (Fig. 3).
Pancreatic transection
The pancreas is transected using an auto-suturing device. The stump of main pancreatic duct is identified in the staple line of remnant pancreas. Using scissors, staples only around the main pancreatic duct are removed and the main pancreatic duct is opened. The pancreatic duct tube as large as possible is inserted as a temporary test tube.
Extracorporeal maneuver: seromuscular excision of the jejunal loop
The jejunal loop is pulled out from a small incision in the umbilicus, and the seromuscular layer at the PJ site is excised. The seromuscular layer of the jejunal loop is repeatedly excised longitudinally (Fig. 4A), and the range is expanded until a sufficient width is obtained to cover the pancreatic stump. A pancreatic duct tube with a nodule is inserted through the middle of seromuscular excision into the jejunal lumen and is reeled out from the site of choledochojejunostomy. The jejunal wall orifice that is as small as possible is created using the metal tip of the tube; it is important to select the largest tube that can be inserted into the main pancreatic duct. Finally, two 12-cm 5-0 polydioxanone sutures with double needles are tied and fixed around the tube (Fig. 4B).
Intracorporeal maneuver
Reconstruction is performed using PD-II. The jejunal loop is pulled up to the pancreatic stump via a retrocolic course. PJ is performed at approximately 15 cm from the jejunal loop stump. First, a 12-mm trocar is inserted in the left epigastrium, immediately in front of the planned PJ position (Fig. 2, ⑥ and Fig. 3, ⑦). For outer-layer sutures, three transpancreatic stitches in a horizontal mattress fashion are placed: Two transpancreatic sutures are placed on both sides as apart from the main pancreatic duct, and the remaining sutures are placed interposing the main pancreatic duct.
First, a double-needle stitch is passed through the jejunal loop from 1 cm behind the seromuscular excision to the posterior edge, which is then crossed over the pancreas at least 1 cm from the stump. Thereafter, transpancreatic stitches are exteriorized through the 12-mm trocar to prevent entanglement (Fig. 4C). The inner-layer suture is also placed in a horizontal mattress fashion with double-ended needles from inside to outside of the main pancreatic duct lumen. The detailed operative procedure using the Kiguchi method is described in Fig. 5. Custom-made 12-cm-long 5-0 non-absorbable monofilament threads with double-ended needles are used to reduce the risk of entanglement in abdominal cavity. Two horizontal mattress sutures, which are placed on ventral (Fig. 6, ①) and dorsal sides (Fig. 6, ②) of the main pancreatic duct, are then held with microvascular clips. Cranial (Fig. 6, ③) and caudal (Fig. 6, ④) sides of the main pancreatic duct are stitched with a single interrupted suture to the pancreatic stump without passing through the lumen. Using one end of each of the four suture needles placed on the pancreatic stump, the jejunal wall around the orifice is stitched one by one and ligated in order, as shown in Fig. 6. Contrary to the conventional duct-to-mucosa anastomosis, in which 6–8 interrupted stitches are placed in a radial direction around the main pancreatic duct, the Kiguchi method utilizes only two horizontal mattress sutures and two interrupted sutures, which are placed to surround the main pancreatic duct in a square pattern and to obtain tight adhesion to the jejunal submucosal layer around the main pancreatic duct using a minimum number of threads. After ligating the thread on the dorsal side (Fig. 6, ②-❷), the tip of the pancreatic duct tube is inserted into the main pancreatic duct (Fig. 4D). The position of the pancreatic duct tube is adjusted and fixed to the anterior wall of the pancreatic duct and the jejunal orifice using the prepared suture threads. During the ligation of inner-layer suture, the pancreatic stump and jejunal loop are approximated by pulling the outer-layer suture threads from outside of the abdominal cavity (Fig. 4E). In the final stage of PJ using the Kiguchi method, ventral edge of the seromuscular layer of the jejunal loop is sutured using horizontal mattress stitches (Fig. 4F). Meanwhile, the pancreatic duct tube is cut off and dropped into the jejunal lumen as a long lost stent.
Selection of operative procedures
In the present study, all patients were evaluated for indications for up-front surgery. The surgery type, OPD or MIPD, was determined based on patient preference, because MIPD was not covered by the national insurance until May 2016. Since June 2016, LPD for benign or low-grade malignant tumors has been covered by the national insurance and patients meeting the criteria tended to choose LPD. RPD was not covered by the national insurance until March 2020, and selection of RPD primarily depended on the patient’s economic conditions. Between January 2008 and August 2016, 19 patients in the Old-MIPD group underwent MIPD with conventional PJ by a single surgeon (IU). Between September 2016 and March 2020, 26 patients in the New-MIPD group underwent MIPD with PJ using the Kiguchi method by two surgeons (IU, GK). Between January 2008 and March 2020, 143 patients in the OPD group underwent OPD with conventional PJ by several pancreatic surgeons with experience of more than 30 conventional PJ cases with OPD, including two surgeons involved in MIPD.
Operative procedures
1. Resection
All patients underwent subtotal stomach-preserving PD. In the New-MIPD group, the novel semi-derotation technique developed by our group was applied for resection, as described in detail elsewhere [18].
2. Reconstruction
In all patients, modified Child’s method was used for reconstruction. The end-to-side PJ was performed at approximately 15 cm distal to the jejunal loop stump in a retrocolic fashion.
3. PJ
OPD group: conventional PJ
Operative procedures in the OPD group were performed through either a midline laparotomy or bilateral subcostal incision. Pancreas was dissected with a scalpel to identify the main pancreatic duct. Interrupted duct-to-mucosa anastomosis was used for PJ in an end-to-side fashion. Cut surface of the remnant pancreas was approximated to the jejunal serosal layer, with three or four interrupted penetrating sutures using the modified Kakita method (Fig. 7) or interrupted horizontal mattress sutures using the modified Blumgart method (Fig. 8) as outer-layer sutures [19, 20]. A duct-to-mucosa anastomosis was formed between the main pancreatic duct and jejunal orifice by interrupted sutures placed in a radial direction using at least six stitches as inner-layer sutures. An external or internal pancreatic duct tube was placed based on the surgeon’s preference.
Old-MIPD group: conventional PJ
Patients were placed in a reverse Trendelenburg position. Five trocars, including three 12-mm and two 5-mm trocars, were used in LPD, whereas five trocars, including two 12-mm and three 8-mm trocars, were used in RPD. Pancreas was dissected with an ultrasonic scalpel to identify the main pancreatic duct orifice. In the Old-MIPD group, all patients underwent conventional intracorporeal PJ similar to that performed in the OPD group. In RPD, inner-layer sutures for duct-to-mucosa anastomosis were performed using at least six single interrupted sutures placed in a radial direction. In contrast, only four single interrupted sutures were performed in LPD because of technical difficulty. An external pancreatic duct tube was placed in all patients.
New-MIPD group: the Kiguchi method
Intracorporeal PJ using the Kiguchi method described above was performed in all patients in the New-MIPD group who underwent surgery via LPD or RPD.
4. Choledochojejunostomy
In all groups, end-to-side choledochojejunostomy was performed using continuous sutures for the posterior layer and interrupted sutures for the anterior layer.
5. Drainage tube management
In all groups, two or three soft silicone drains were indwelled around the PJ.
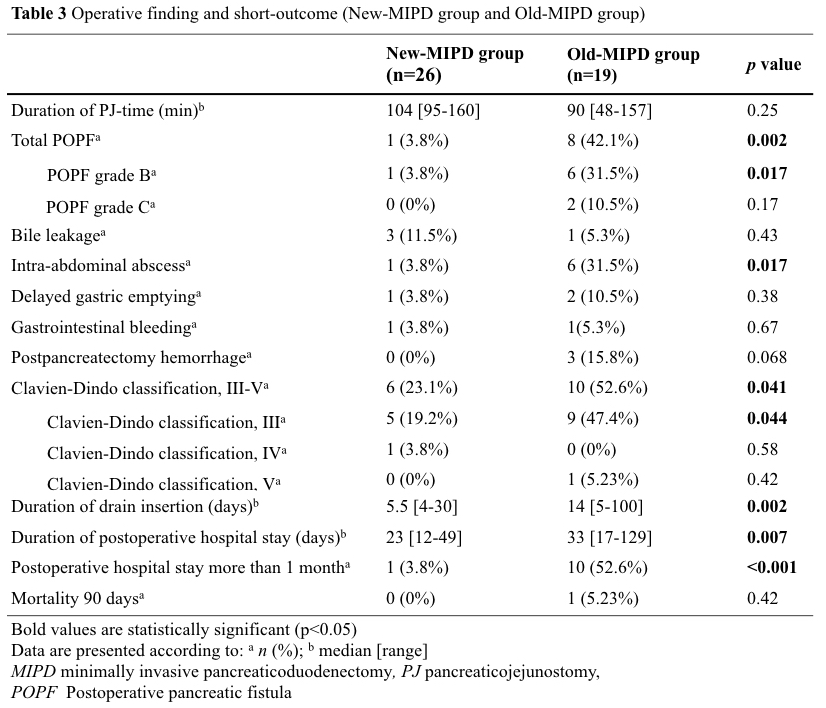
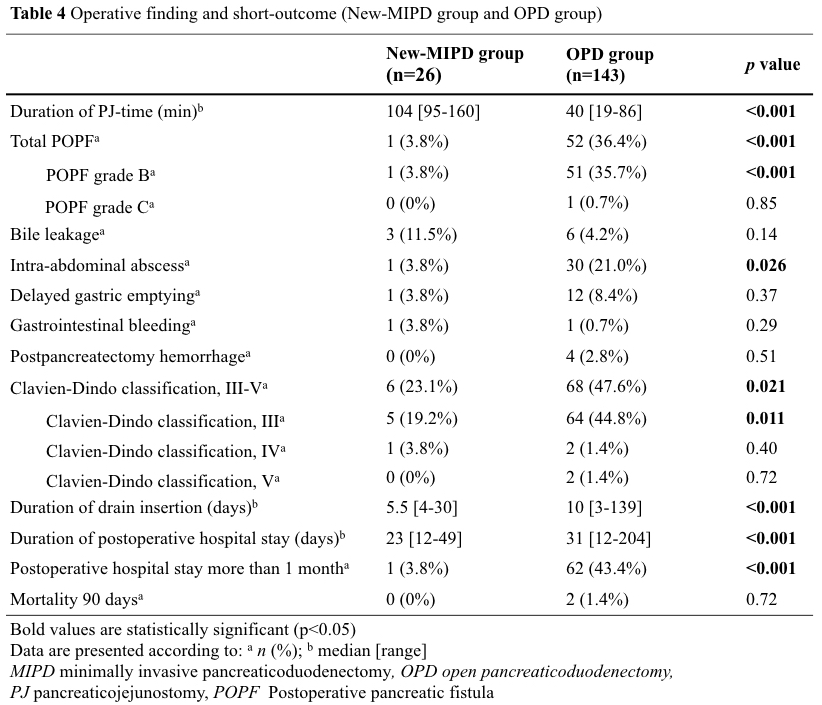
Patients were treated in the intensive care unit for at least one day before their transfer to the general ward. For POPF diagnosis based on the International Study Group on Pancreatic Surgery (ISGPS) definition, amylase concentration via the drainage tube was measured daily for a minimum of three days after surgery. The drainage tube was removed on postoperative day 3–7 in the absence of drain effusion as evidence for POPF. In patients with POPF, the drainage tube was exchanged at the appropriate timing until the drainage fluid became negligible.
Study outcomes
The following clinical characteristics were analyzed: use of robotic surgery, age, sex, body mass index, American Society of Anesthesiologists physical status score, main pancreatic duct diameter, presence of malignancy, use of biliary drainage, and presence of diabetes mellitus as a comorbidity. A main pancreatic duct with a diameter of <3 mm was defined as narrow. The operative and postoperative data in the present study included PJ length, postoperative complications, duration of drain indwelling, and postoperative hospital stay.
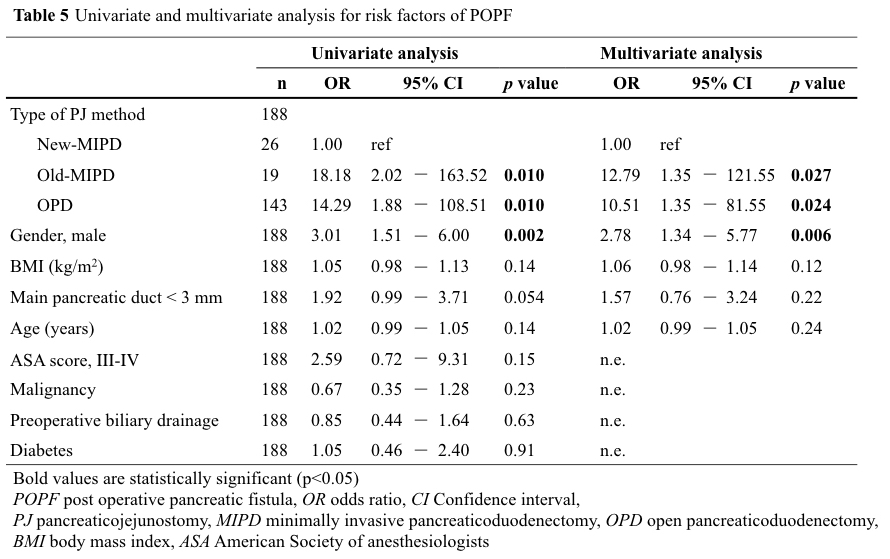
Postoperative complications were defined according to the Clavien-Dindo classification [21]. POPF, one of the most important postoperative complications of PD, was classified in accordance with the 2016 ISGPS guidelines [22]. Postoperative surgery-related complications were determined according to the ISGPS definitions [23, 24]. Postoperative mortality was defined as death occurring within 90 postoperative days. Grade B/C POPF was defined as the primary endpoint for univariate and multivariate risk factor analyses.
Statistical analysis
Continuous variables were presented as medians with range (minimum to maximum), and categorical variables are reported as numbers and percentages. The New-MIPD group was compared with the Old-MIPD and OPD groups using Pearson’s chi-squared test for categorical variables and the Mann-Whitney U test for continuous variables.
A p value of less than 0.05 was considered to indicate statistical significance. All preoperatively parameters significantly correlating with POPF were included in a multivariate binary logistic regression model. All statistical analyses were performed with SPSS version 23.0 for Windows (Statistical Package for the Social Sciences, Chicago, IL).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}