The role of surgery in patients who achieve cCR after nCRT is controversial. This systematic review and meta-analysis showed that nCRT alone has better survival benefit compared with nCRT plus surgery. There was no significant difference in DFS (HR = 1.19, 95% CI = 0.41–3.46). This survival benefit in nCRT may be attributed to the lower mortality in the nCRT group than in the nCRT plus surgery group and the pattern of failure between nCRT and nCRT plus surgery. Specifically, nCRT plus surgery showed better local control, but it also showed a higher incidence of distant failure than nCRT.
Currently, nCRT plus surgery is the preferred approach for locally advanced operable esophageal cancer. One study showed that salvage esophagectomy provides patients with LR a chance for long-term survival[19]. CRT alone is also a feasible option for these patients, and several studies showed that there is no benefit in the addition of surgery[5–7]. Thus, it raises the question of whether surgery is of benefit in locally advanced operable esophageal cancer. Particularly, in the case of complete responders after nCRT, who are known to have low recurrence rates and high survival rates[20], omitting surgery could be more beneficial because it avoids the morbidity and mortality associated with the addition of surgery. Wilk et al. retrospectively compared the treatment outcomes between active surveillance and immediate surgery in patients with cCR after nCRT[18] and found that although there was no statistical difference, the survival rates were higher in the active surveillance group (3-year OS = 77% vs. 55%, p = 0.10; 3-year progression-free survival (PFS) = 60% vs. 54%, p = 0.87). Meanwhile, a recent prospective study showed that nCRT is associated with a higher relapse rate and a lower survival rate (HR = 1.17, p = 0.28 for PFS; HR = 1.48, p = 0.56 for OS)[12]. The cCR rate was 47.6%, which is approximately 7% higher than Wilk’ study. However, the two studies differed in assessment of cCR, as the former used bite-on-bite biopsy, and the latter performed a regular biopsy. Results from the recently published preSANO study revealed that compared to regular biopsies, the sensitivity for the detection of residual disease increased substantially from 54–74% with bite-on-bite biopsies[21]. We could presume that inclusion of more patients with false-negative results could cause a detrimental effect on the analysis of treatment outcomes of nCRT.
Thus, the important issue is the accuracy of cCR for predicting pathologic CR (pCR) and its reliability as an indicator for omitting surgery in cCR after nCRT in esophageal cancer. Endoscopy or endoscopic ultrasonography (EUS) with biopsy, computed tomography (CT), and positron emission tomography (PET)-CT are generally used to evaluate treatment response after nCRT. However, no single modality could produce satisfactory results. A meta-analysis on accuracy of modalities showed pooled sensitivities and specificities of 33% and 95% for endoscopic biopsies, 96% and 8% for qualitative EUS, 74% and 52% for qualitative PET, 69% and 72% for PET using maximum standardized uptake value (SUVmax), and 73% and 63% for PET using percentage reduction of SUVmax, respectively[22]. A systematic study reported that the negative predictive value of negative endoscopy biopsy after CRT was only 47%[23]. Cheedella et al. reported the result of response evaluation after CRT using endoscopy with biopsy and the maximum standard uptake value of PET-CT[24]. The sensitivity of cCR for pCR was 97.1%, and the specificity was 29.8%. They concluded that cCR is not highly associated with pCR due to the low specificity. However, magnetic resonance imaging (MRI) is emerging as a promising method for response evaluation as it was highly predictive of histopathologic response and has the potential benefit of a multiparametric approach using diffusion-weighted and dynamic contrast-enhanced image[25, 26]. A recent prospective study reported that PET and MRI are effective in predicting pathologic response[27]. In addition, this study reported that a combined model of MRI, PET, and histology could improve the predictive rate compared to using each modality alone (c-statistic 0.84 vs. 0.79).
Surgery has a major impact on the patient’s quality of life (QOL). Boehier et al. investigated long-term QOL and symptom evolution up to 20 years after esophagectomy[28] and found that esophagectomy was associated with decreased QOL and lasting gastrointestinal symptoms up to 20 years after surgery. Meanwhile, CRT negatively affects the QOL during treatment, but it is mostly recovered after. Noordman et al. reported that a negative impact of nCRT on QOL was observed only during the last cycle of CRT and up to 2 weeks after CRT[29]. Physical functioning, odynophagia, and sensory symptoms were restored to baseline levels from 1 to 2 months after nCRT. Odynophagia, fatigue, and weight loss improved after nCRT within 4 months.
In this study, the risk of treatment mortality was lower in nCRT than in nCRT plus surgery. However, this does not include mortality after salvage surgery in cases of LR in nCRT. Several previous studies report that patients who receive salvage surgery have high morbidity and mortality, with anastomosis leakage occurring in 21–38% and the mortality ranging from 4–33%. Meanwhile, survival was similar to that of patients who received planned surgery[30–34]. However, these results should be interpreted with caution due to the inclusion of inoperable patients who received high-dose radiotherapy (> 60 Gy). Notably, the morbidity and mortality have been greatly reduced in decade, and the differences of those between planned and salvage surgery have also been reduced. In the MD Anderson Cancer Center, comparison between the early era (1987–2000) and modern era (1997–2010) showed that the mortality rate decreased from 6–3% for planned surgery and from 15–5% in salvage surgery[35]. Indeed, better survival in nCRT may reflect advancements in surgical technique, lower dose of radiotherapy, and selection of patient with cCR.
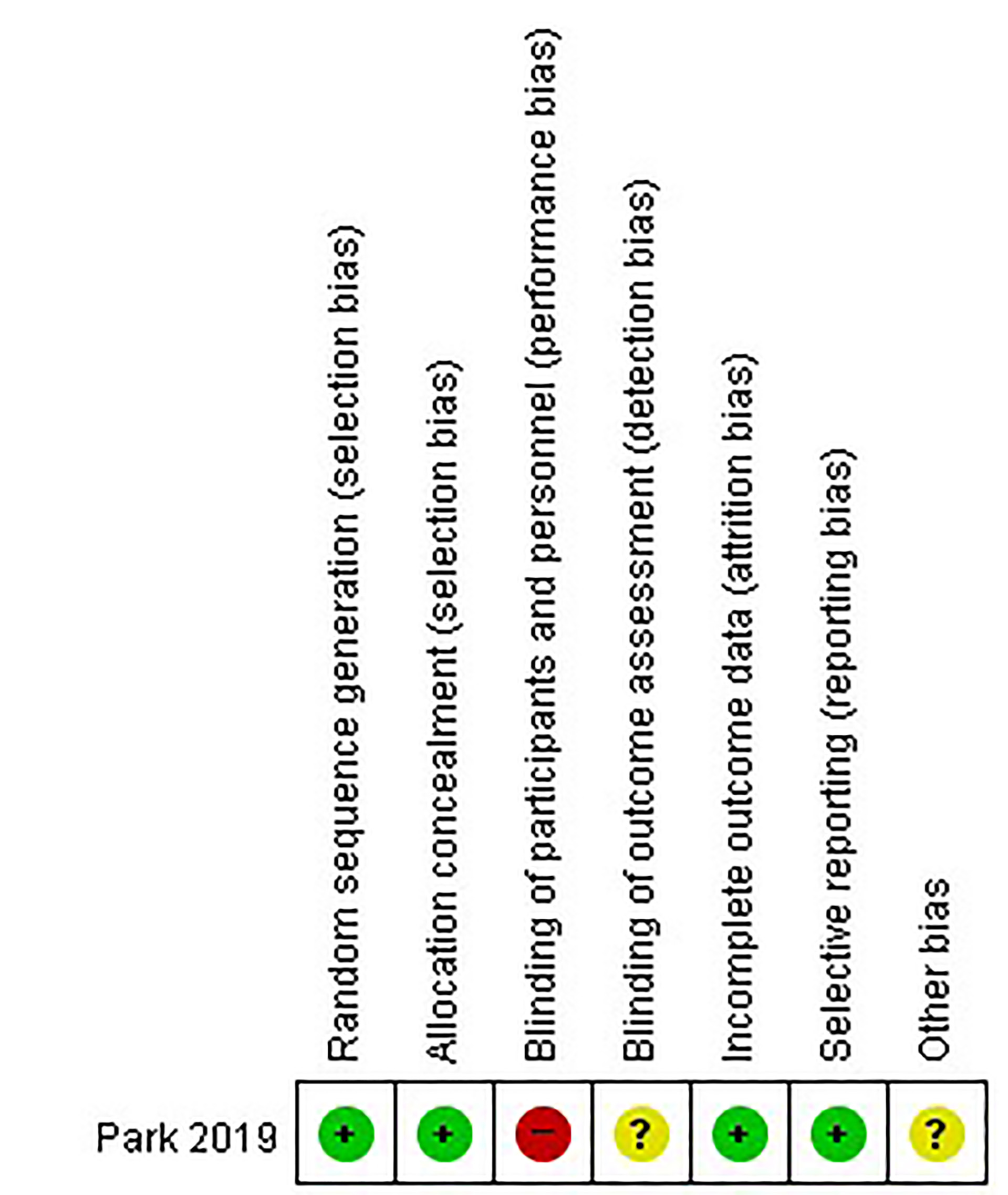
This study has some limitations that should be considered when interpreting the results. First, five of the six studies selected were retrospective. Thus, selection bias could be inevitable between nCRT and nCRT plus surgery, and cofounding factors cannot be balanced. Second, the analysis of long-term outcomes was limited survival data only up to 2 years were included in the analysis. However, there may be little difference in the survival tendency because most recurrence occur within 2 years. Current large prospective studies such as the SANO- and ESOSTRATE-trials will resolve this limitation. Third, subgroup analyses of esophageal ACC and SCC could not be performed because all included studies did not provide treatment result according to histology. Most patients in this meta-analysis had SCC, which is generally known to be more sensitive to chemoradiotherapy. Although there is no significant difference in complete response rates between ACC and SCC (median 22.0% [range, 9.0–40.0%] vs. 23.7% (range, 16.0–41.0%)[36], further research on the feasibility of omitting surgery after nCRT in ACC is needed. Further prospective randomized controlled clinical trials with large sample sizes are also needed to validate our findings.
{kind=link}