In present study, all methods were carried out in accordance with Human Subjects Research Act and informed consent was obtained according to Scope of Human Clinical Trials Exempted from Informed Consents of Subjects in Ministry of Health and Welfare, Taiwan (R.O.C.). The ethical approval was obtained by Institutional Review Board of Kaohsiung Medical University Memorial Hospital (KMUHIRB-E(II)-20190406). The study protocol conformed to the principles outlined in the German Ethics Committee’s statement.
Eighty-four extracted permanent teeth were collected, including 36 anterior teeth, 24 premolars, and 24 molars. All teeth were extracted due to periodontal disease, but endodontically treated teeth and teeth with extensive decay or restoration were excluded. All teeth were mounted in six stone models, including three maxillary models and three mandible models, according to their anatomic position from central incisor to second molar.
For all models, preoperative CBCT with a voxel size of 150 µm was performed (NewTom VGi evo, CEFLA, Imola, Italy), and data were saved in Digital Imaging and Communication in Medicine (DICOM) format. Furthermore, the models were scanned with an intraoral scanner (3Shape TRIOS, 3Shape, Copenhagen, Denmark), and surface data were saved in the stereolithography (STL) file format. Both types of data were superimposed in dental CAD software (Implant Planning, Inteware, Chiayi, Taiwan) for virtual access cavity planning.
The endodontic access bur (Munce Discovery Bur #1/4, Hager & Meisinger GmbH, Neuss, Germany) was used for virtual access cavity planning. This bur has a tip diameter of 0.5 mm, shank diameter of 1 mm, and a working length of 16 mm. A virtual image of burs 0.5 mm in diameter was planned using the software, and a virtual bur was placed 3–4 mm below the cementoenamel junction with the axial within the range of the conservative endodontic access cavity (Fig. 1a). Of the 84 teeth, 36 virtual burs were positioned in anterior teeth, 33 burs in premolars, and 48 burs in molars. In anterior teeth, all canals were planned. In premolars and molars, canals with complexity were excluded. For example, mesiobuccal root in upper molar with first and second mesiobuccal canal, C-shape root canal in premolar and molar were excluded to prevent the misjudgement of canal accessibility.
After virtual planning, the templates were designed using software (Guide Designer, Inteware, Chiayi, Taiwan; Fig. 1b), and all resin sleeves in templates were designed with a 1.09-mm inner diameter and a 3-mm sleeve height (Fig. 1c). Twelve templates were created in STL file format and fabricated with a 3D printer (Form 2, Material: FLGPGR04, Formlabs, Somerville, USA). After the support material of the templates was removed, a fit checking material (Fit Checker, GC Corporation, Tokyo, Japan) was used for all templates.
All models were mounted in dental simulation units (DSE Expert, KaVo Dental GmbH, Biberach, Germany) with the opposite jaw model to simulate the clinical situation and operated by a single endodontic specialist. Enamel within the area of the conservative access cavity was removed with a round diamond bur until the dentin was exposed, and templates were then attached to the models. The bur was used with a low-speed handpiece to penetrate through the sleeve of the template with a pecking motion until the bur hit the mechanical stop of the resin sleeve. The bur was cleaned with gauze, irrigation with sodium hypochlorite was performed every 2 mm during drilling, and the bur was replaced every 10 canals. After guided access cavity preparation was completed, each canal was checked with a size 10 K-file (Dentsply Sirona, Charlotte, USA) to evaluate the canal accessibility. If the K-file could reach the root canal through guided access cavity preparation without any resistance, the procedure was deemed a canal accessibility; otherwise, it was deemed a canal inaccessibility. After canal accessibility was recorded, root canal negotiation was performed with ultrasonic tips (CPR®, Obtura-Spartan Corp., Fenton, MO) and K-files under a microscope (OPMI pico, Zeiss, Oberkochen, Germany) from the guided access cavity.
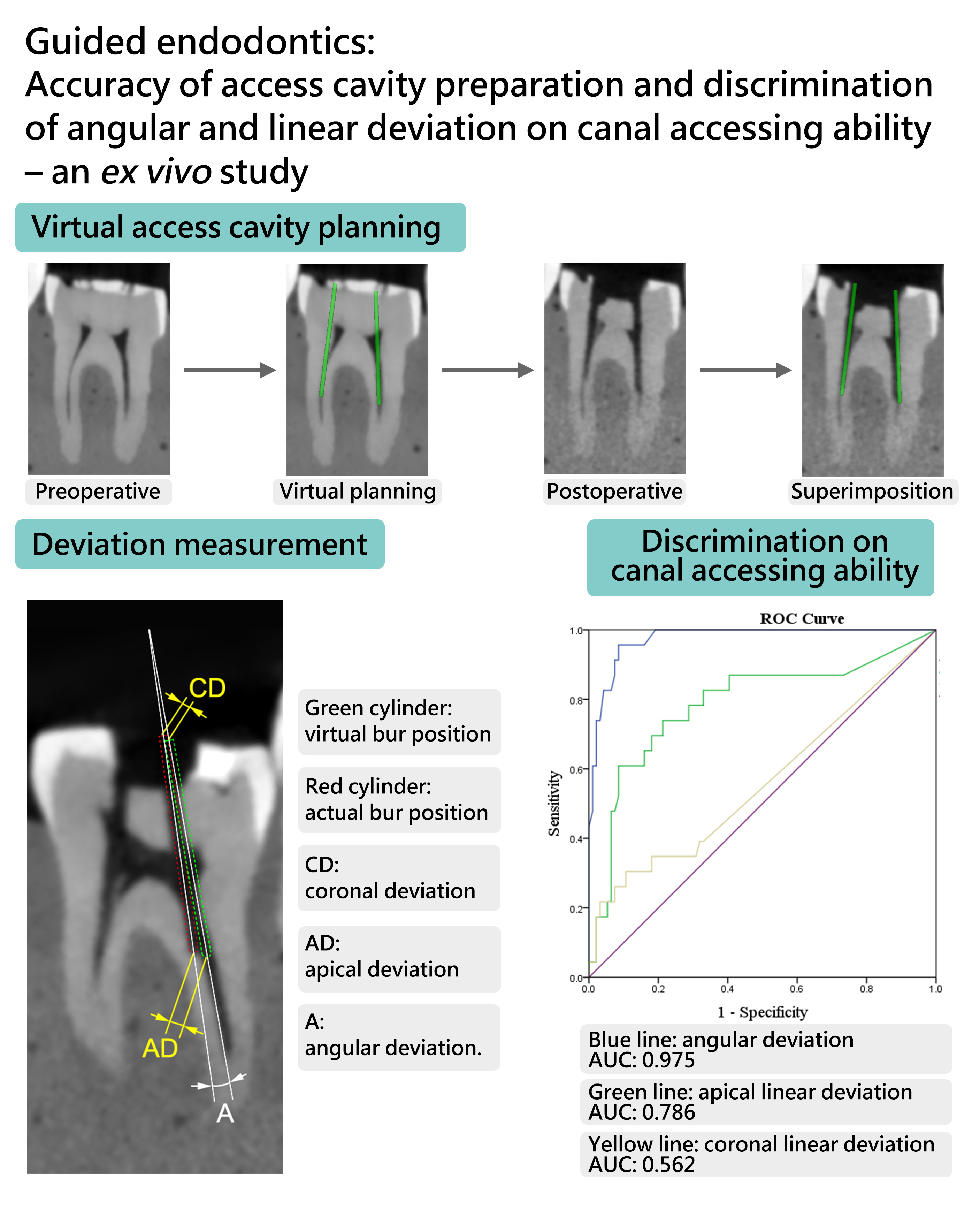
Postoperative CBCT of all models was performed. All data, including those of preoperative and postoperative CBCT, oral scans, and virtual planning, were imported and superimposed (Fig. 2) in a 3D slicer (available at http://www.slicer.org/). The angular and linear deviations were measured in a 3D view. The angle between the virtual bur axis and the actual bur axis was defined as angular deviation. The distance between the bases of the virtual bur and actual bur was defined as coronal deviation, and the distance between the tips of the virtual bur and actual bur was defined as apical deviation, and the angle between the axis of virtual bur and actual bur was defined as angle deviation (Fig. 3).
Teeth were categorised into three groups: anterior teeth (AT), premolar (P), and molar (M). Statistical analysis was performed with SPSS v20 (IBM, New York, USA). Nonparametric statistics were used, and the significance level was set at 5% (P < 0.05). Receiver operating characteristic (ROC) curves were used to evaluate the predictive ability of angular and linear deviation for canal accessibility.
{kind=link}