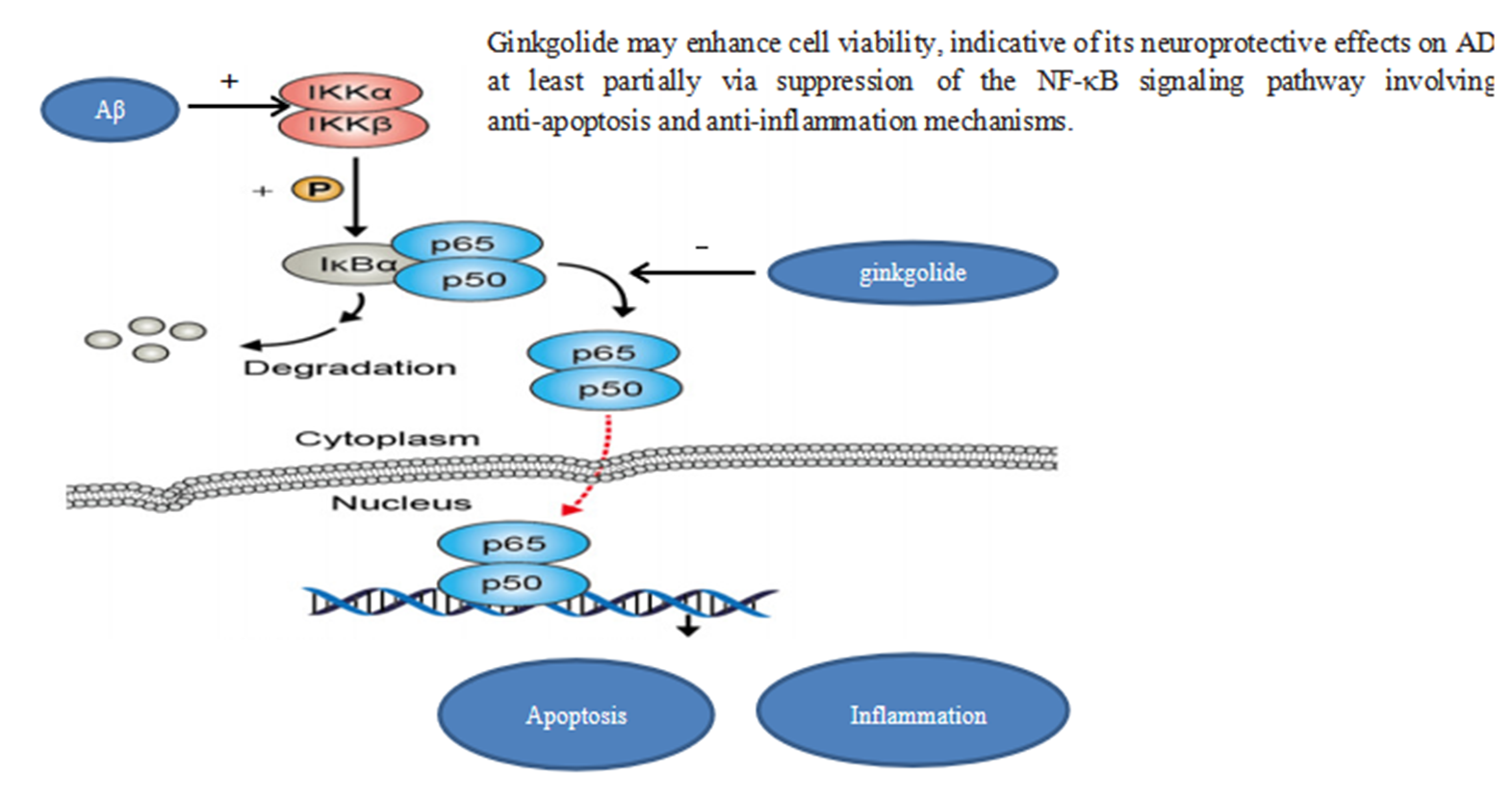
As one of the most prevalent neurodegenerative disorders, Alzheimer’s disease (AD) is characterized by irreversible cognitive impairment and memory loss, with the accumulation of amyloid-beta (Aβ) and neurofibrillary tangles, which represent typical pathological features [1]. Increasing evidence has substantiated that the Aβ-induced inflammatory response plays a crucial role in the neurodegenerative process of AD, and Aβ-mediated neuroinflammation is predominantly regulated via the nuclear factor kappa B (NF-κB) signaling pathway [2–4]. As a ubiquitously expressed transcription factor in eukaryotic cells of the nervous system, NF-κB family transcription factors function as master regulators of immune development, immune response, inflammation, cancer, and apoptosis [5, 6]. Such activities are mediated through homo-or heterodimerization of NF-κB subunits RelA/p65, RelB, c-Rel, p50, and p52, of which RelA/p65 is the most abundant subunit [7]. Proteins of the inhibitory κB (IκB) family function as inhibitors and regulators of NF-κB activity. Members of the IκB family include the classical IκB proteins (IκBα, IκBβ, and IκBε), NF-κB precursor proteins (p100 and p105), and nuclear IκBs (IκBζ, Bcl-3, and IκBNS). Upon stimulation of innate immunity receptors, such as Toll-like receptors and the cytokine receptor tumor necrosis factor receptor superfamily, a series of membrane-proximal events cause the activation of IκB kinase (IKK). Phosphorylation of IκBs contributes to their proteasomal degradation, the release of NF-κB for nuclear translocation and activation of gene transcription, consequently leading to inflammation and immune response [8, 9]. Recent studies have confirmed that NF-κB signaling has a key regulatory role in the pathogenesis of AD, and hence, it has been considered a compelling target for therapeutic intervention [10, 11].
Currently, both cholinesterase inhibitors (donepezil, carbazatin, and galanthamine) and N-methyl-D-aspartate receptor antagonists (memantine) are recommended to treat AD. However, these medications are not ideal because their therapeutic effects are accompanied by adverse effects. Although numerous new agents for the treatment of AD have been developed, such as aducanumab and crenezumab [12], they have not been fully implemented in clinical practice because of a lack of definitive therapeutic effects. GV-971, a marine algae-derived oral oligosaccharide, has been approved for clinical use, but its efficacy remains disputable [13]. In the past decade, botanical preparations with multi-target treatment and high-level safety have become a new trend in the research and development of therapeutic drugs for AD. Various in vivo and in vitro studies have reported the interventional effects of botanicals, such as resveratrol, Rhodiola sachalinensis, curcumin, and natural polyphenols on AD, suggesting their therapeutic potential for the prevention and treatment of AD [14–17].
As a botanical agent, Ginkgo biloba (GB) extract has been widely used to treat cerebrovascular diseases because of its multiple biological and pharmacological activities, such as antioxidative, anti-inflammatory, and anti-allergic effects as well as free radical scavenging and platelet aggregation suppression [18, 19]. Interestingly, several recent studies have revealed that GB extracts also exhibited certain therapeutic effects on dementia. Given these findings, GB extract has been recommended for the treatment of AD patients, especially for those who have failed to benefit from other treatments [20]. Currently, the international standard extract of GB is EGb 761, produced according to the German Schwabe patent process. EGb 761 is a well-defined plant extract product of Ginkgo biloba leaves. The extract contain two main active substances: flavonoid glycosides (24–26%) and terpene lactones (6–8%) consisting of ginkgolides A, B, C, and bilobalide [21]. Furthermore, based on technological advances, a new product of ginkgolide (Baiyu®), which is composed of ginkgolide ABCJ and bilobalide, has been recently developed and approved for the treatment of ischemic cerebrovascular disease; however, its therapeutic efficacy in the context of AD remains unclear. Hence, we performed a preliminary study to investigate the effects of ginkgolide (Baiyu®) and its components (ginkgolide B and bilobalide) on cell viability in an AD cellular model involving an APP/PS1 double gene-transfected HEK293 cell line (APP/PS1-HEK293) and further explored the related mechanisms of action.
{kind=link}