We carried out a multi-method, ToC-driven evaluation of GCC’s 2012-2016 global mental health investment portfolio. This portfolio consists of 56 mental health projects funded through the Global Mental Health and Transition to Scale programmes. Our objectives were:
- To describe the characteristics of the mental health projects included in the GCC portfolio.
- To assess the extent to which grantees achieved their pre-identified outcomes on a collective pathway of change.
- To illustrate the use of a multi-method ToC-driven methodology as a means of synthesising key data and learning regarding the implementation of a diverse portfolio of projects.
- To investigate, using qualitative methods, factors affecting implementation that may help or hinder progress along the pathway of change (reported elsewhere in this series).
Evaluation Framework
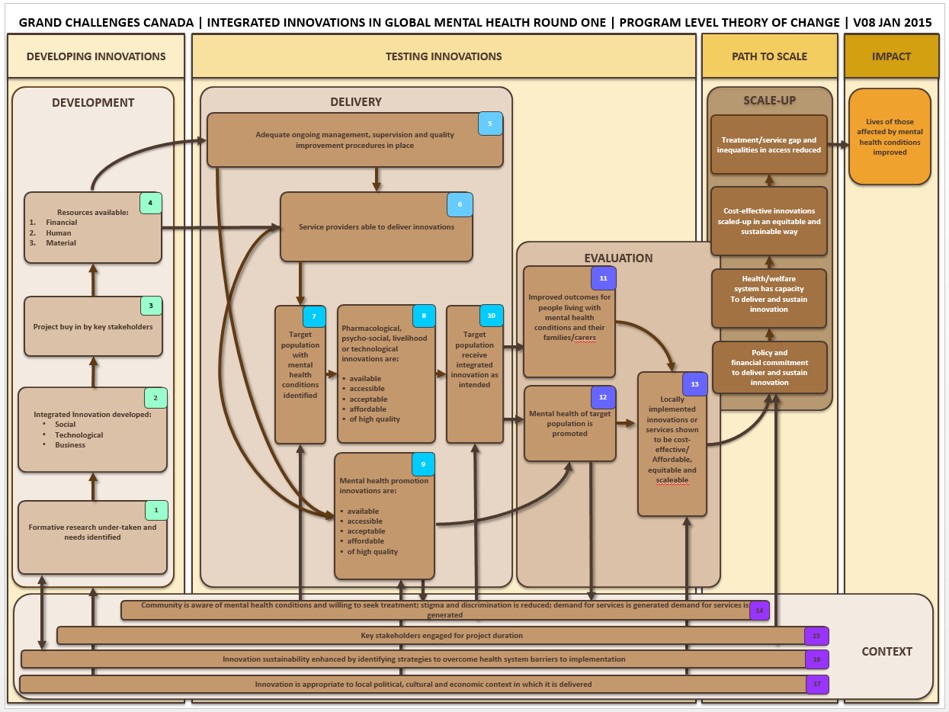
Portfolio-Level Theory of Change
From 2013 to 2016, GCC funded an innovator support platform called the Mental Health Innovation Network (MHIN, www.mhinnovation.net). MHIN is a collaboration between the Centre for Global Mental Health at the London School of Hygiene and Tropical Medicine (LSHTM) and the Department of Mental Health and Substance Abuse at the World Health Organization (WHO). One of the key services that MHIN provided to GCC was assistance in portfolio-level monitoring and evaluation.
To evaluate the collective impact of mental health projects across GCC’s funding programmes, researchers at MHIN proposed a ToC-driven approach. ToC is “a theory of how and why an initiative works”, laying bare the causal pathway by which an initiative aims to achieve impact (18). Often a ToC is depicted visually as a diagram and developed in consultation with key stakeholders, with additional benefits for consensus-building and communication (15, 21). By assigning indicators to short-, medium- and long-term outcomes along the causal pathway, a ToC can be especially valuable as an evaluation framework. Pin-pointing where on this causal pathway an initiative fails to produce expected outcomes can help to “unpack the black box” of evaluation (22), distinguishing between “ideas that don’t work” (theory failure) and “ideas that haven’t been properly tested” (implementation failure)(23).
At the time of GCC’s Global Mental Health Programme launch, ToC was already in use by international mental health research consortia like PRIME (PRogramme for Improving Mental hEalth care) (24). Utilizing a combination of country-specific and overarching, cross-country ToC maps, PRIME demonstrated that it is possible to simultaneously monitor and evaluate necessarily heterogenous, complex interventions both at the individual country level and collectively across participating country sites. PRIME’s Nepal site has also demonstrated that ToC can be used in combination with methods of qualitative comparative analysis (QCA) to identify which conditions are necessary and sufficient to bring about change (25)
In international development more broadly, ToC is increasingly being used by funders to plan, monitor and evaluate their portfolios (17, 18, 22, 26). A ToC can be empirically tested and amended iteratively to reflect new learning, providing a road-map for current and future investment (18, 22, 26, 27). Funders may be encouraged to develop an a priori ToC map before starting the selection process, to gauge how each potential applicant can contribute to the envisioned pathway of change (17, 22). However, particularly in relatively young fields such as global mental health, grantees may have more specialist expertise and experience than their funders (17, 22). Under these circumstances, grantees can play an important role in defining the pathway by which they expect the funding they receive to help achieve the funders’ desired impact (17, 22). In the case of GCC, a ToC was developed through an iterative process involving grantees and representatives of the funding organisation, facilitated by experienced evaluators from the MHIN team at LSHTM.
Development of the Theory of Change
An initial ToC workshop was held at a Grand Challenges Community Meeting in Rio de Janeiro, Brazil, in October 2013. A working statement of impact was agreed and outcomes were backward-mapped onto a ToC diagram [Appendix 1]. Indicators were suggested for each outcome under a proposed ceiling of accountability, defined by De Silva et al. (2014, p. 5) as the level at which you “stop accepting responsibility for achieving those outcomes… often drawn between the impact and the long term outcome”. Because only a very small proportion of GCC grantees would go on to receive funds for “Transition to Scale”, this ceiling of accountability was drawn under “Scale-Up”.
Grantees also received training and elective one-to-one support to develop their own project-specific ToC diagrams. These were compared to the portfolio-level ToC, which was then revised accordingly. Further adjustments were made upon review of grantees’ ‘Core Metrics’ reporting (described below), again to ensure that the portfolio-level ToC adequately reflected the component projects. Revisions to the portfolio-level ToC were presented to grantees and representatives of the funding organisation during annual GCC meetings, for feedback. Final changes were made in April 2015, at which point the ToC was “locked” for evaluation.
Data Collection
As GCC already had a mandatory RMAF reporting system in place, proposed portfolio-level ToC indicators were adjusted where possible to align with existing indicators. The goal was to minimise the burden of reporting placed on grantees, while still collecting data against essential process and outcome indicators for monitoring and evaluation of the overall portfolio. The result was a Core Metrics Framework introduced in early 2015, consisting of 23 indicators linked to the 17 outcomes of the ToC map [Appendix 1]. These outcomes were grouped under four domains: project development (n=4), delivery (n=6), evaluation (n=3), and context (n=4). For each indicator relevant to their project, the grantee was asked to set a target prior to the start of implementation, then report results (for example the number of people they expected to treat through the project). Reports were submitted by grantees to GCC and transferred to MHIN at six-month intervals for analysis.
Analysis
The quantitative analysis was conducted between November 2016 and March 2017. We used the latest available data from all GCC projects (n=56) related to delivery outcomes [Table 1]. We used descriptive statistics to describe the projects’ characteristics, results based on indicators and to compare projects’ level of achievement in relation to their intended targets. All analyses were conducted using IBM SPSS Statistics (Version 25).
Our analysis plan was affected by several data limitations, despite numerous efforts to contact grantees both directly and via GCC to verify project data. First, large amounts of data were missing, mainly because not all outcomes were applicable to all projects. However, it was not always possible to differentiate between data that were missing due to irrelevance and data that were missing due to purposeful or accidental omission or inadequate monitoring and evaluation. Missing data was a particularly big issue for the project development outcomes. Second, given that many grantees did not report data on the outcomes of service users or other beneficiaries (e.g. family members) within the GCC-funded timeframe, most of the data collected against the Core Metrics Framework were related to implementation. Some grantees never completed their evaluations of beneficiaries’ outcomes, and others were protective of their results during the long embargo period for publication in peer-reviewed journals. Third, our quantitative approach was ill-fitted to some of the more heterogeneous outcomes that proved difficult to categorise (e.g. outcomes related to context) and were better described through rich qualitative descriptions. Due to these challenges, we limited our quantitative analysis to delivery outcomes [Table 1].
In the analysis of service delivery data, there were several instances when disaggregated data was not provided by grantees (e.g. for types of providers trained or types of diagnoses screened, diagnosed and treated). Regarding types of diagnoses, several projects targeted more than one disorder therefore in the absence of disaggregated data it was impossible to know the number of people that had been screened, diagnosed or treated in each category. We only present disaggregated data when available and report the number for which disaggregated data is not available.
|
Table 1. Summary of indicators for delivery outcomes
|
|
Outcome
|
Indicator
|
|
1. Adequate ongoing management, supervision and quality improvement procedures in place
|
Continuous quality improvement (CQI) mechanism in place (e.g. regular supervision, repeat training, other CQI methods)
|
|
2. Number of service providers (intermediaries) trained
|
Numerator: Number of service providers (intermediaries) trained
Denominator: Target number of service providers (intermediaries) to be trained
|
|
3. Target population (beneficiaries) with mental health disorders identified
|
Numerator: Number of people in target population (beneficiaries) screened and identified
Denominator: Target number of people to be screened and identified
|
|
4. Health promotion innovations are accessible
|
Numerator: Proportion of target population with access to innovation medium (e.g. television, radio, internet)
Denominator: Expected proportion of target population with access to the innovation medium (e.g. television, radio, internet)
|
|
5. Target population (beneficiaries) receive integrated innovation as intended
|
Numerator: Number of people (beneficiaries) who received innovation (disaggregated by diagnosis, level of care, year of project etc.)
Denominator: Target number of people to receive innovation
|
{kind=link}