Experimental studies suggest that microbiota, microbial products (like SCFA) and the intestinal immune system might be involved in the pathogenesis of MS. Hitherto, only sparse clinical data exist. In this study, we investigated fecal markers related to intestinal inflammation in RRMS patients and age-matched controls.
Contrary to what we initially hypothesized, fecal calprotectin concentrations, a robust and sensitive marker even for subclinical intestinal inflammation, was in the normal range in the majority of investigated RRMS patients and there was no difference regarding fecal calprotectin concentrations between RRMS and control subjects. While there is one study reporting elevated calprotectin concentrations in the cerebrospinal fluid of MS patients (20), fecal calprotectin concentrations have not been reported for MS previously. Normal fecal calprotectin concentrations could be caused by the fact that most investigated RRMS patients were under immunotherapy, which beside their effect on the CNS alter enteric inflammatory processes, as well. Consequently, the observation of normal fecal calprotectin concentrations in our RRMS cohort might be explained by this effect, in particular 14 of the RRMS patients were treated with natalizumab, a drug also administered in Crohn’s disease(21).
Assuming that immunotherapies in MS exert anti-inflammatory effects also in the gastrointestinal tract, the intestinal microbiota (as indicated by Storm-Larsen et al. for dimethylfumarate (27)) and subsequently intestinal SCFA production might be affected as well. Hence, the lack of a significant difference between RRMS patients and controls with regard to fecal SCFA concentrations in this study might also be explained by a drug effect.
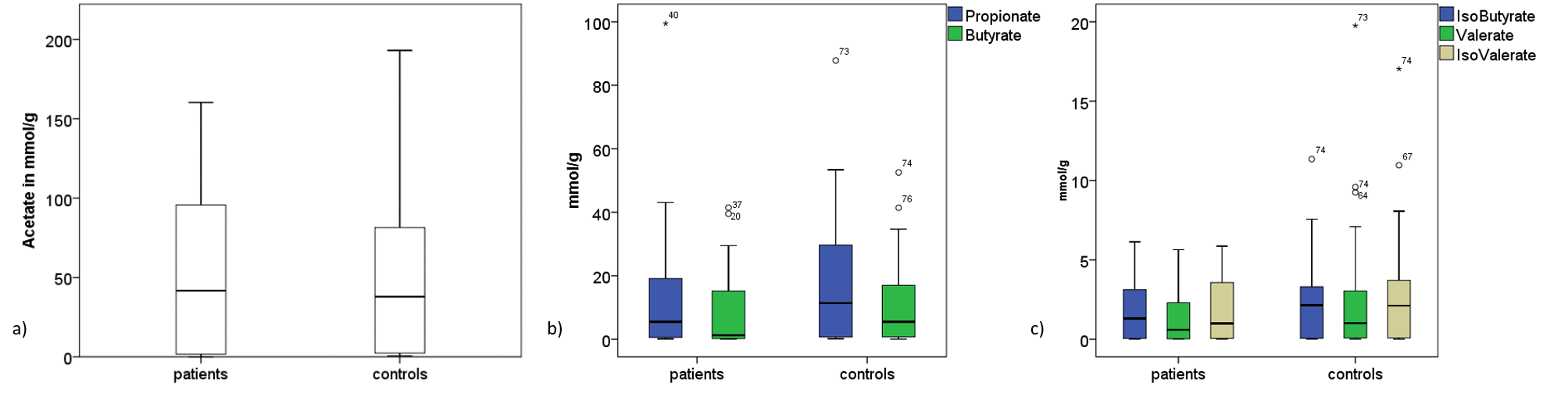
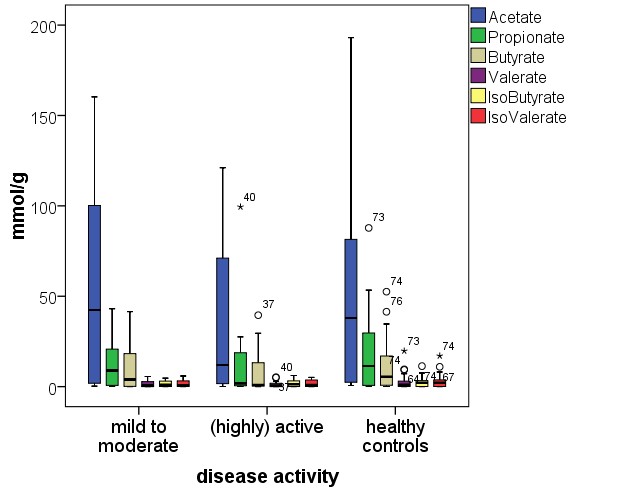
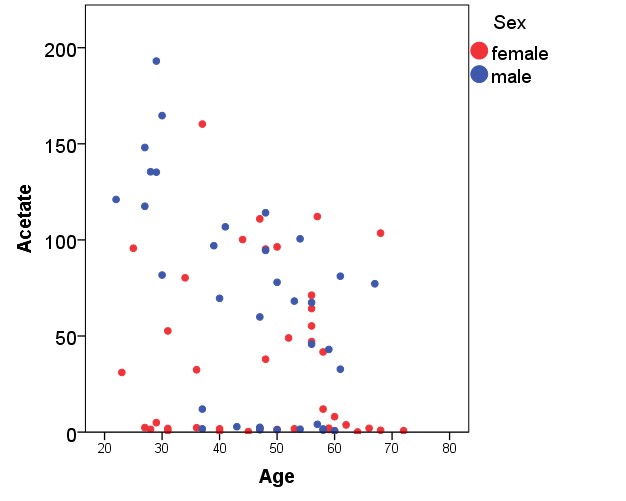
Despite the lack of a statistical significance, we observed descriptively lower fecal SCFA concentrations in RRMS patients compared to controls, especially for butyrate. This descriptive finding is in line with the few studies investigating SCFA in MS: Park et al. showed, that SCFA blood concentrations were reduced in MS patients (14). A Chinese study reported reduced fecal SCFA concentrations in MS patients (13). An altered intestinal microbiota has been reported in MS patients as well (22–24). Moreover, the highly significant correlation of fecal SCFA concentrations with age in controls, but not in patients, endorses the assumption that either MS or MS therapeutics affect gut microbiota metabolism.
Recently, the potential clinical relevance of SCFA in MS has been investigated in a clinical trial (6): Duscha et al. reported an enhancement of Treg differentiation, reduced autoinflammation and improvements in the clinical course of MS after oral administration of propionate (6). It is important to note that orally administered SCFA are absorbed to a great extent in the small intestine. SCFA produced by the gut microbiota in the colon mainly exert local effects and are unlikely to affect systemic SCFA concentrations as effective as an oral supplementation.
We are not able to draw conclusions concerning fecal calprotectin and SCFA concentrations in drug-naïve MS patients as the vast majority of our RRMS cohort was under immunotherapy. As the investigated RRMS patients were under different treatment regimes, we also analyzed subgroups of RRMS patients defined by the therapeutic regime. Yet, the number of subjects per subgroup was rather small and the study population was not treated with the full spectrum of available MS therapies. Large-scale longitudinal studies, including drug-naïve MS patients are necessary to distinguish between disease-immanent and therapeutic effects on intestinal inflammation, intestinal microbiota and microbial products, like SCFA, in MS. Another interesting topic for future investigations is the role of (subclinical) intestinal inflammation as a trigger for relapse in MS
An unexpected finding of our study was the marked sex-associated difference in SCFA concentration between women and men with significantly lower SCFA concentrations in female subjects. Sex-specific differences have been described for the intestinal microbiota previously (25). Fecal SCFA concentrations have already been subject of clinical studies in different fields, e.g. anorexia (29), obesity, diabetes mellitus and cardiometabolic disease (30). Yet, none of these studies reported sex-specific differences for fecal SCFA concentrations. It might well be that this aspect was not explicitly analyzed in these studies.
Jakobsdottir and colleagues reported sex-specific differences of blood SCFA concentrations (with lower SCFA concentrations in female subjects) in a study comparing patients with microscopic colitis and celiac disease (26). Another study did not find sex-specific differences when analyzing blood SCFA concentrations (27). As already mentioned, blood and fecal SCFA concentrations are not directly comparable.
In addition, potential confounding factors such as dietary habits, need also to be investigated. Patients and controls in this study were matched in terms of age, but there was a male predominance in the control group, which represents a potential confounder.
Taken together, the known female predominance in MS and the known immunomodulatory effects of SCFA warrant further studies in this field. One might hypothesize that low concentrations of SCFA represent an additional risk factor for MS and might contribute to the higher susceptibility of women compared to men in MS. As the observed sex-specific difference in SCFA concentrations was independent from MS, also studies in other conditions that investigate microbiota and microbial products should consider sex as a potential confounder.
{kind=link}
{kind=link}
{kind=link}