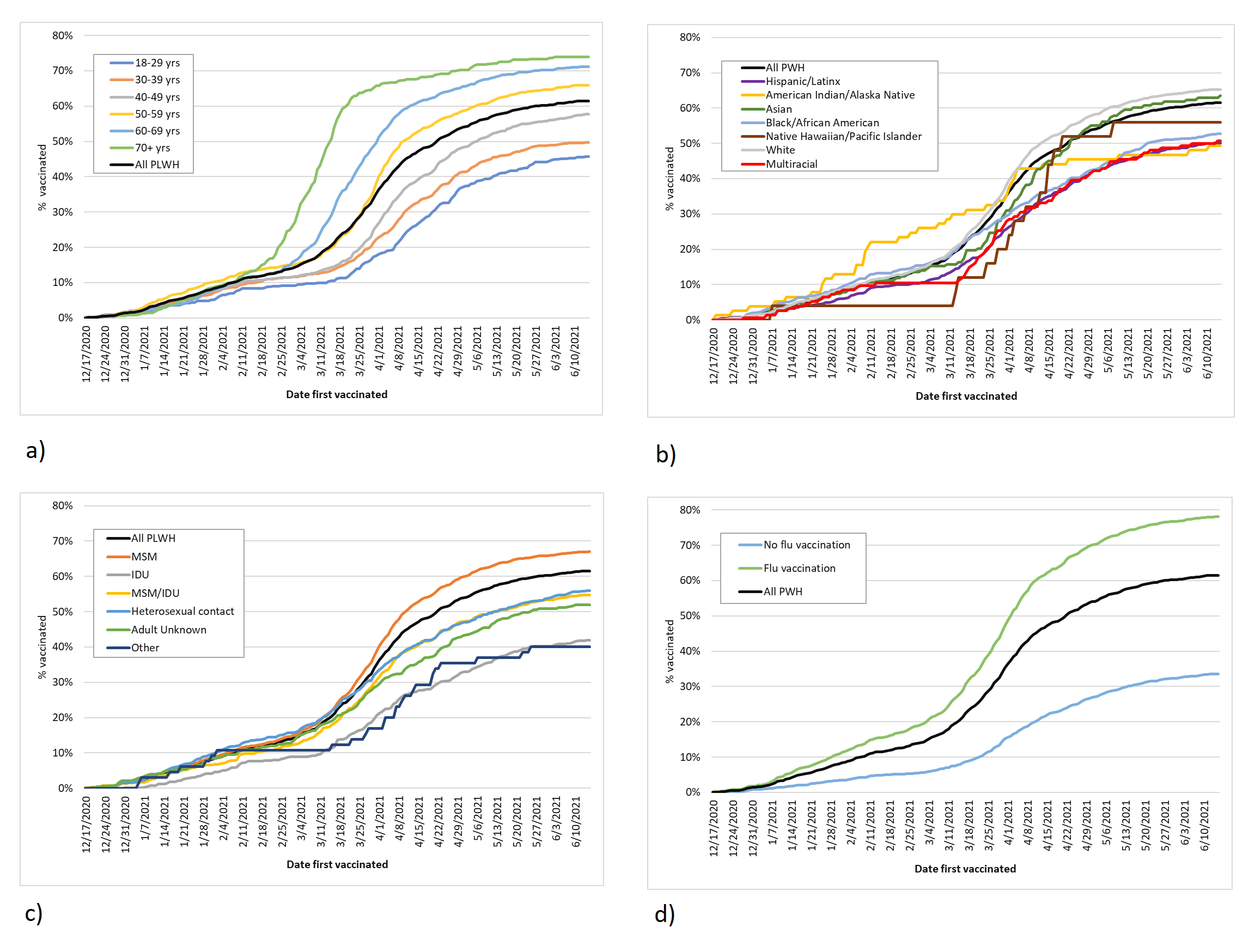
Just over three-fifths of PLWH in Oregon received at least one dose of a COVID-19 vaccine as of June 15, 2021. While COVID-19 hospitalizations are increasing among younger adults,9 COVID-19 vaccination uptake was lowest among PLWH 18–29 years old. Early vaccine eligibility prioritized older adults but a quarter of younger adults reported that they would probably or definitely not get vaccinated citing concerns about safety and side effects.10 PLWH of color overall, and Hispanic/Latinx PLWH in particular, were less likely to be vaccinated compared to white PLWH. Building trust in COVID-19 vaccination among PLWH of color requires not only coordinated, broad-based grassroots vaccine advocacy, but also authentic community investment that acknowledges experiences of racism in health care.11 Vaccine uptake among PWID was low. Harm reduction programs have proven essential during the COVID-19 pandemic and the integration of vaccination into syringe service programs may be key to enhancing vaccine access and uptake among PWID. In addition, PLWH in rural and frontier areas, where vaccine availability is sparser and vaccine hesitancy is higher,12 were less likely to be vaccinated compared to PLWH in urban areas.
PLWH who did not have a CD4 count or viral load in 2020, a proxy for care engagement, were less likely to be vaccinated than those who did. Many clinics deferred routine care for patients with well-controlled HIV and/or converted to telemedicine. For some PLWH, the risk of COVID-19 made attending clinic unsafe. Expansion of home- and community-based vaccination programs may improve vaccine uptake among PLWH whose access to in-person care has been curtailed by COVID-19. Moreover, vaccine uptake was lower among those at greater risk of severe COVID-19 as defined by viral load and CD4 counts.1 In addition, PLWH with lower CD4 counts may mount an inadequate response to vaccination and may require increased support to complete a newly recommended three-dose vaccination series for people with untreated or advanced HIV. Social determinants of health affecting uptake of COVID-19 vaccination likely overlap with those affecting clinic attendance, antiretroviral adherence, and viral suppression.5 In contrast, ADAP enrollment was associated with greater vaccine uptake; case managers facilitate access to vaccination through assistance with finding vaccination sites, appointment scheduling, and transportation. Finally, receipt of influenza vaccine was the strongest predictor of COVID-19 vaccine uptake as PLWH vaccinated against influenza likely have more confidence in the effectiveness and safety of vaccines.
There are limitations to this work. First, ALERT IIS only captures vaccines administered in Oregon; therefore, PLWH vaccinated out of state were not represented in these data. Second, reporting to ALERT IIS may not be 100% complete resulting in missing vaccination status for some PLWH. Third, because HIV surveillance does not collect clinical data on comorbidities, it was not possible to examine vaccine uptake by comorbidities that may increase COVID-19 risk. Finally, measurements of CD4 count or viral load reported to the surveillance system were a proxy for care engagement. The presence of these measurements may represent either an in-person visit, a telemedicine visit with an associated laboratory visit, or just a laboratory visit. Each type of care engagement may have differential impact on vaccine uptake that is not captured in these data.
COVID-19 vaccination is critical to the survival of PLWH through this novel global pandemic. Younger PLWH, Hispanic/Latinx PLWH, PWID, who live in rural and frontier areas, who have not engaged in care or enrolled in ADAP, and who have not received an influenza vaccine may benefit from more intensive advocacy, outreach, and care navigation to increase COVID-19 vaccine uptake.
{kind=link}