In the present study, in agreement with our hypothesis that CVP may be an intermediary that delivers pressure from PEEP to ICP, we found that ICP was increased after PEEP only with baseline ICP close to CVP, i.e. PICGap was narrower in the responder group compared with the non-responder group (1.63±1.33 versus 6.55±2.46 mmHg). This indicates that the same increment of CVP (4.39±1.30 versus 4.25±1.58 mmHg) could obliterate PICGap in the responder group, but not in non-responders (Figure 1). We also evaluated whether PICGap, baseline ICP, and baseline CVP could predict ICP responsiveness to PEEP in patients with sTBI. The results suggested that PICGap was the strongest predictive indicator among the three parameters. PICGap less than 2.5 mmHg could predict ICP responsiveness to PEEP tuned up to 15 cmH2O. To the best of our best knowledge, this is the first study demonstrating that PEEP-induced changes of ICP depend on PICGap rather than PEEP itself.
Although cerebral hemodynamics is not governed entirely by extradural venous pressure since normal ICP (8-13 mmHg) is higher than the venous pressure outside the dura (0-5 mmHg), the changes of extradural venous pressure transfer to the brain circulation might rely on a certain situation [22]. The degree of subdural venous collapse was related to the difference between ICP and extradural venous pressure, and this passive collapse acts as a variable venous outflow resistance. An alteration of extradural venous pressure causes up- or downregulation of venous outflow resistance through the self-regulation of the degree of passive collapse according to the Starling resistor model [23].
CVP could act as a surrogate marker of extradural venous pressure, because the pressure falling on the jugular vein is negligible in the supine position. A preliminary experiment also showed that CVP values were the same as those of jugular bulb pressure. According to the Starling resistor model [23], once the value of CVP after PEEP exceeds baseline ICP, venous outflow resistance would be downregulated to the lower limit. In such a situation, the brain circulation would be impeded, with ICP rising accordingly.
The relationship between PEEP and CVP has been validated by previous studies. Stepwise PEEP elevation induces an increase of CVP [17]. An increase of 12 cmH2O in PEEP caused a more than 4 mmHg rise of CVP in the current study, which was consistent with previous findings [17]. Thus, it is reasonable to infer that PEEP directly increases CVP, and whether CVP after PEEP could increase ICP depends on the extent of PICGap narrowing by CVP.
The lower the PICGap, the easier it is for CVP after PEEP to exceed baseline ICP; then, the Starling resistor would lose effectiveness as a result of the elimination of venous outflow resistance. As indicated in Table 1, patients with responsiveness to PEEP adjustment had relatively lower PICGap compared with the non-responder group. Thus, based on the hypothesis that CVP is an intermediary which connects PEEP to ICP, we found that PICGAP, a new indicator, could provide a rational explanation regarding the underlying mechanism, which also accounts for the individual heterogeneity proposed by Yang and colleagues [15].
Brain compliance is unfavorable in patients with sTBI because of cerebral edema associated with injury. In this case, cerebral venous return impeded by increased CVP after PEEP would contribute to increasing ICP after PICGap is narrowed to zero. A study by Robba and colleagues investigated the effects of pneumoperitoneum and the Trendelenburg position on ICP in non-brain injured patients (lower ICP), and demonstrated that both increase ICP [24]. There was no significant change in arterial blood pressure and CPP in the study. Although CVP was not monitored, increased ICP might be due to an obstruction of cerebral venous return theoretically [25].
Several studies used baseline ICP to predict the responsiveness of ICP to PEEP, and found that patients with lower baseline ICP have a positive response to various PEEP levels [26, 27]. These results were consistent with our findings. Individuals with elevated mean baseline ICP experienced no significant changes of ICP during PEEP alteration. However, these studies have not clarified that a certain ICP value could predict ICP responsiveness to PEEP. Our results also showed that baseline ICP was not a more efficient predictive indicator compared with PICGap.
It should be mentioned that ICP responsiveness to PEEP may be influenced by compliance of the respiratory system [28, 29]. Assessment of patients with low-compliance lungs showed that cerebral hemodynamics and ICP are not influenced by the application of PEEP, because less compliance may not transmit the increased pressure to the entire intrathoracic space effectively. In the current study, all the enrolled patients had normal compliance (Table 1). In addition, recent studies have challenged the effects of PEEP on ICP, arguing that PEEP may be more related to eventual changes in hemodynamics or lung compliance than affecting CVP [30-32]. For example, it was proposed that ICP markedly increases after PEEP application, but only in case PEEP induces alveolar hyperinflation with subsequent PaCO2 increase [30].
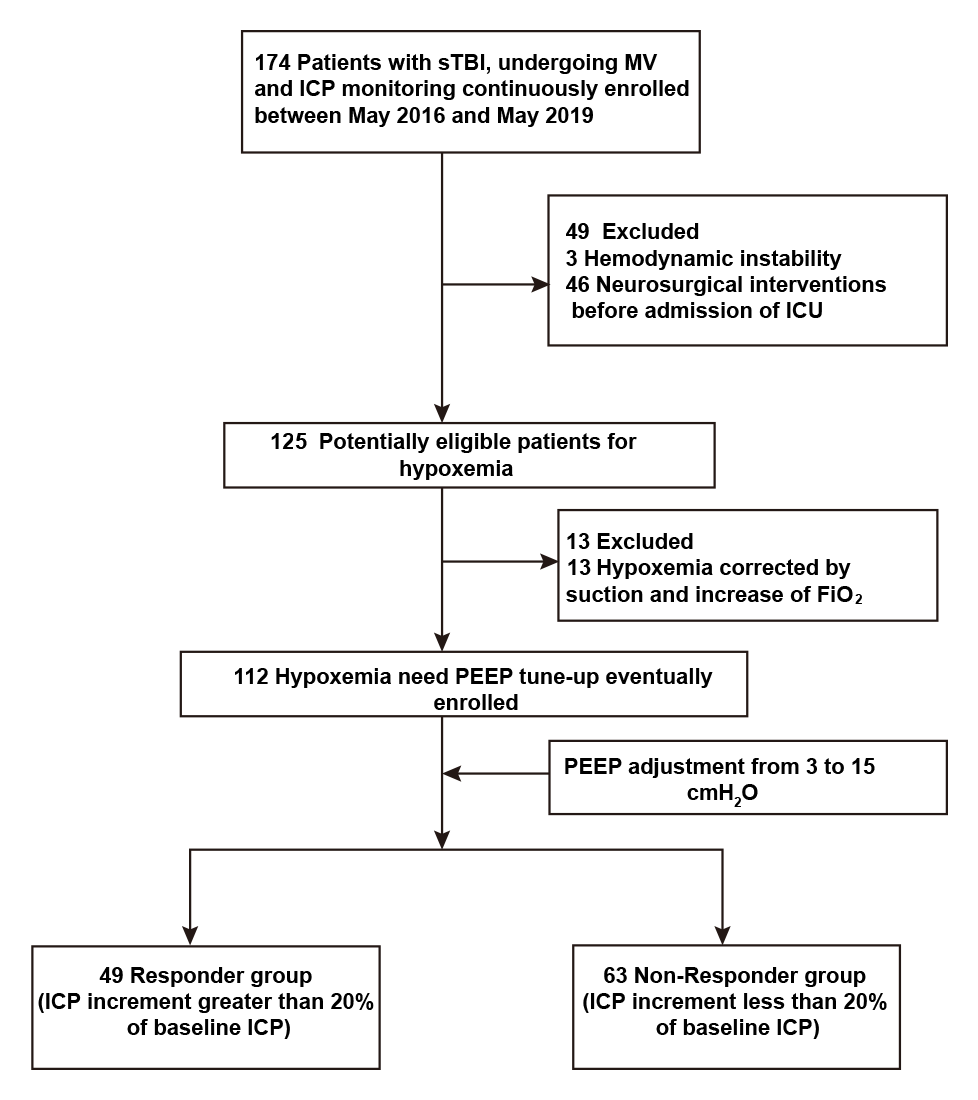
It is known that sTBI patients tend to progress rapidly early after injury; therefore, they were kept in the ICU for 24 hours after injury for close monitoring of ICP in this study. To prevent catheter-related infections, the ICP monitoring probe was implanted for no more than 7 days. In case of hypoxemia, increased PEEP was provided for lung recruitment and increased oxygen saturation. The purpose of a PEEP of 15 cmH2O during lung recruitment was to avoid the harmful effects of high PEEP (>20 cmH2O), such as worsened hemodynamics and significantly increased ICP. Consequently, no serious complication was recorded in this study (Table E1). In addition, maintaining PEEP at 15 cmH2O for 2 minutes helped achieve pulmonary bloating [20] and normalize PetCO2 to avoid the impact of CO2 retention on ICP [21]. PEEP in this study did not adversely affect hemodynamics in both patient groups (Table E1), and there was no significant difference in prognosis between the two groups (Table E2).
The limitations of this study should be mentioned. First, the sample size was relatively small for a clinical study. In addition, the effect of PEEP on CBF was not evaluated. However, we maintained PetCO2 at the normal level, and ICP elevation was in a permissible range, indicating likely stable CBF. Furthermore, although PICGap is a dynamic marker, it did not change dramatically in the early stage of TBI in certain patients after neurosurgery, ensuring the predictive value individually.
{kind=link}