Study Design: This was a single-center interventional study, in which patients were assigned to change the D[Ca] from 1.75 mmol/L (standard-calcium) to 1.25 mmol/L (low-calcium) for one year.
Glucose concentration, inflow volume, and the number of exchanges a day were responsibilities of the physician in charge. Physicians were free to adjust the dose of dialysis and medications to maintained mineral and bone biomarkers within the recommended target.
Setting: stable adult patients on PD were recruited at the Hospital das Clinicas HCFMUSP, Universidade de Sao Paulo, Brazil, in the period between December 2017 and March 2020.
Participants: the inclusion criteria were patients > 18 years old who were on PD for at least 3 months. The exclusion criterion was severe hypocalcemia (total calcium < 7.5 mg/dl).
The local Research Ethics Board of the Hospital da Clínicas da Universidade de São Paulo (Cappesq# 30284714.0.0000.0068) has approved the study protocol. All participants provided written informed consent to participate in the study.
Variables of interest were etiology of renal disease, age, weight, blood pressure, presence of comorbidities such as hypertension and diabetes mellitus, history of coronary and cerebrovascular disease, active medications, time on PD, and type of dialysis. We also collected data on residual diuresis, renal kt/V, and body composition, assessed by electrical bioimpedance. Biochemical variables evaluated included total and ionized calcium (tCa and iCa), phosphorus (P), 25(OH)-vitamin D, PTH, alkaline phosphatase (ALP), and hemoglobin (Hb).
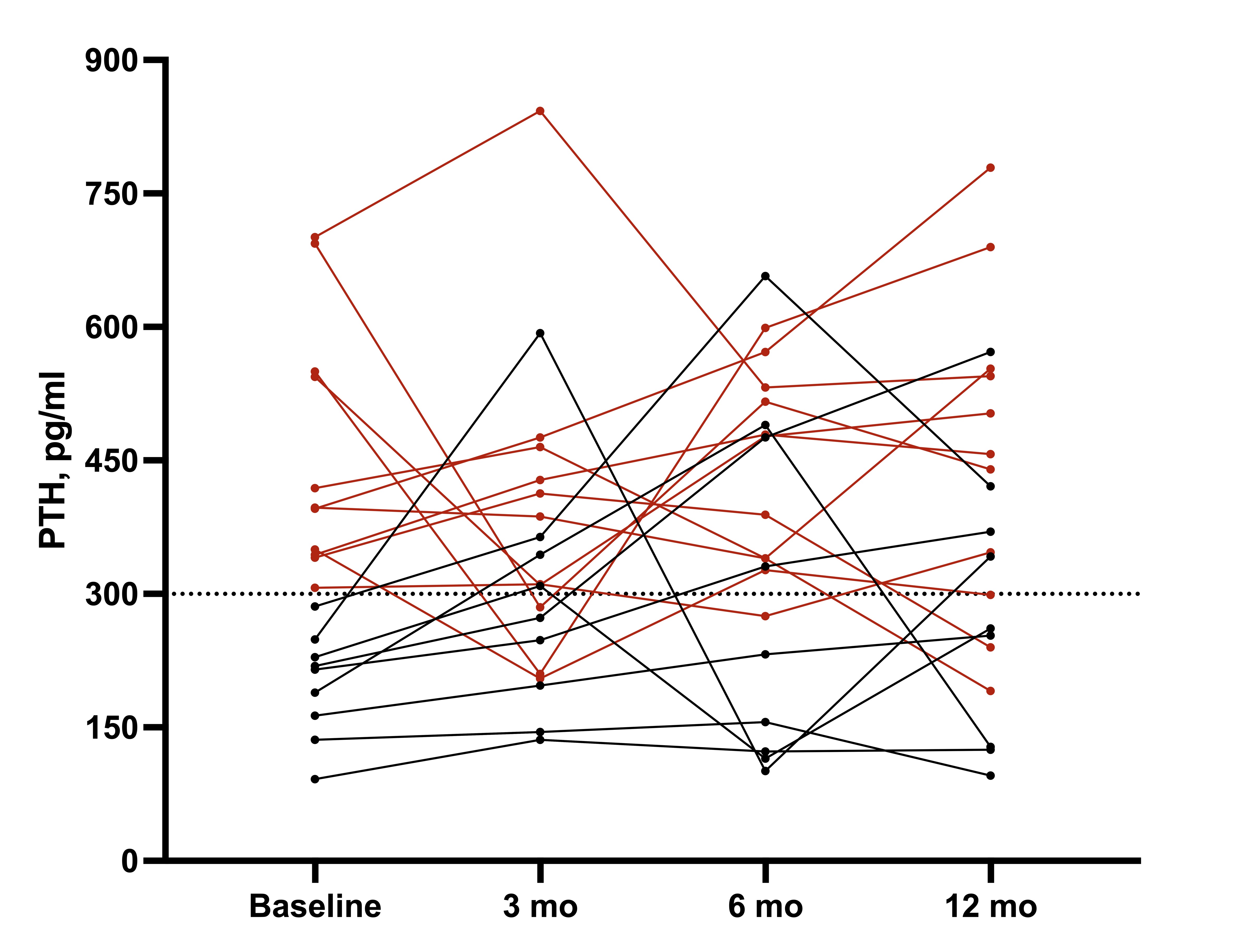
The outcomes evaluated were changes in PTH, tCa, iCa, P, vitamin D, and ALP levels. These markers were assessed at baseline, 3, 6, and 12 months after the intervention.
Laboratory Measurements: all biochemical analyses were done according to the manufacturer’s instructions and usual techniques. Hb was measured using Laser/spectrophotometry (Reference range – RR: 13.5–17.5 g/dl for men and 12.0-15.5 g/dl for women), tCa and P were measured by colorimetric method (RR 8.4–10.2 mg/dl, and 2.7–4.5 mg/dl, respectively), iCa was measured by an ion-selective electrode (RR 4.73–5.29 mg/dl); ALP was measured by colorimetric method (RR 35–104 U/L in women and 40–129 U/L in men); 25OH-vitamin D was measured by chemiluminescence (RR 30–100 ng/ml). PTH was measured by chemiluminescence immunoassay (RR 11–65 pg/mL; Roche immunoassay analyzer, Roche Diagnostics, Germany).
Bias: to minimize the bias, the same observer collected biochemical data e follow the medical consultations to assure adherence to the prescribed drugs.
Study size: adopting PTH levels as the main outcome, the required sample size to reach 5% of alpha error and 80% of power was calculated in 18 patients, in a repeated-measures study design.
Statistical analysis: the results are presented as the mean ± SD or median and (25, 75) quartiles depending on the normality of the data, tested by Shapiro-Wilk. General linear model (GLM) repeated measures procedure was used to test the effect of reduction in D[Ca] on variables of interest. P-value obtained described the within-subject difference (baseline, 3, 6, and 12 months). When Mauchly’s test of sphericity was violated (p < 0.05), we used the Greenhouse-Geisser correction. The correlation coefficients were Pearson or Spearman, depending on the normality of the data. A p-value < 0.05 was considered significant.
Analyses were performed with the use of SPSS 21.0 (SPSS Inc., Chicago, Ill., USA) and GraphPad Prism® software version 7.0 (GraphPad Software, Inc., Calif., USA).
{kind=link}