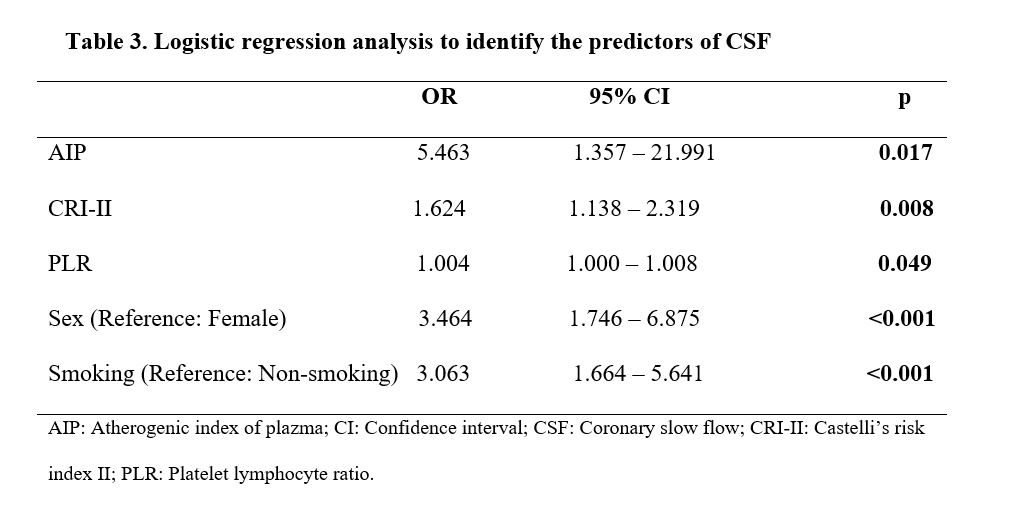
This study was performed to investigate the relationships of CSF with traditional lipid parameters and atherogenic indices (e.g., AIP, AC, CRI-I, and CRI-II) that have been associated with increased cardiovascular risk. Atherogenic indices were higher and HDL-C values were lower in patients with CSF, compared with the control group. AIP, CRI-II, current smoking, and male sex were found to be an independent risk factor for CSF. In addition, LDL-C and non-HDL-C values were significantly higher in the CSF group compared to the control group.
In CSF, washout of the contrast agent is prolonged in the absence of any spasm, thrombus, dissection, and any stenosis that causes significant occlusion in epicardial coronary arteries. Although the incidence of CSF in diagnostic coronary angiography is not rare, its pathogenesis has not yet been well elucidated. Various mechanisms have been proposed for its etiology, including subclinical diffuse atherosclerosis. Cin et al. [13] examined the coronary arteries of 19 patients with CSF using fractional flow reserve and intravascular ultrasonography. They noted extensive calcification and diffuse intimal thickening along the vessel walls and atheroma plaques that did not cause lumen narrowing in patients with CSF, as well as diffuse atherosclerosis in the microvascular system and epicardial coronary arteries. Pekdemir et al. [14] reported diffuse intimal thickening and calcifications along epicardial arteries during coronary angiography examinations of patients with CSF. Ding et al. [15] reported that lipoprotein-associated phospholipase A2, which plays a role in inflammation and atherosclerosis in the vessel walls, was significantly and independently associated with the presence of CSF. Considering the data obtained from these studies, it may be reasonable to conclude that diffuse coronary atherosclerosis plays a role in the etiopathogenesis of CSF.
Atherogenic dyslipidemia, which is present in metabolic syndrome, insulin resistance, type 2 diabetes mellitus, and visceral adiposity, indicates an increased risk of cardiovascular disease in these patient populations [16, 17]. High levels of TG and low HDL-C levels in plasma are typical in patients with atherogenic dyslipidemia, although LDL-C levels are normal. In addition, increases in the levels of plasma very-low-density lipoprotein and small dense LDL-C, and reduced clearance of apolipoprotein B-containing particles from plasma have been identified in patients with atherogenic dyslipidemia [18]. Compared with other LDL subfractions, small dense LDL particles are more atherogenic because they are more susceptible to oxidative stress and can pass through the subendothelial space more easily due to their small diameter. Accordingly, they can stay in circulation longer and have less affinity for LDL receptors [19]. With regard to the origin of small dense LDL formation, Berneis et al. [20] proposed that TG-rich lipoproteins (e.g., very-low-density lipoprotein 1) are converted into small dense LDL after delipidation by hepatic lipase and lipoprotein lipase enzymes. The Framingham Heart Study showed that small dense LDL level is directly correlated with serum TG level and inversely correlated with serum HDL-C level in patients with metabolic syndrome [21]. It was suggested that the TG/HDL-C ratio could be used as an indicator of LDL subfraction [22]. There is increasing evidence that both predominance and elevated levels of small dense LDL-C play important roles in the initiation and progression of atherosclerosis, as well as increased risk of cardiovascular disease [19, 23, 24]. In a recent meta-analysis of 21 studies, Liou et al. [25] reported positive associations of small dense LDL level and cholesterol content of small dense LDL with the risk of coronary heart disease. These findings are supported by an increasing body of evidence in favor of the causal link between small dense LDL and coronary heart disease. However, because the test to measure small dense LDL is complex and costly, its measurement is unlikely to be applicable in routine clinical practice [26].
AIP, calculated as log10 (TG/HDL-C), is regarded as an indirect indicator of small dense LDL-C [7]. Wang et al. [2] described a strong correlation between AIP and syntax score in patients with coronary heart disease. In a prospective observational study of women > 60 years old, a negative correlation between HDL-C concentration and AIP was founded, but observed a positive correlation between all-cause deaths and AIP, after adjusting for age, smoking, and statin therapy [27]. AIP was significantly associated with an increased risk of coronary artery calcification progression beyond that conferred by traditional risk factors [28]. In a study conducted in 1059 patients with a history of acute coronary syndrome before the age of 35 years, the presence and severity of acute coronary syndrome were found to be independently associated with AIP, and these relationships were stronger than those of simple lipid parameters (i.e., TC, TG and LDL-C) [29]. TG/HDL-C ratio, AIP and CRI indices have predicted cardiovascular events better than traditional lipid profiles such as LDL-C and non-HDL-C [30].
To our knowledge, there have been no studies regarding the relationship between CSF and AIP. In the present study, we identified a positive correlation between AIP and TIMI frame count, which is regarded as an indicator of coronary flow reserve. The predictability of TIMI frame count by AIP supports the role of diffuse atherosclerosis in the pathophysiology of CSF. The results of the present study showed that AIP provided a reference for CSF severity. In addition, LDL-C and non-HDL-C, which are defined as the main indicator of atherogenic particles by current guidelines, were higher in the CSF group than in the control group. However, these lipid parameters were not found as predictive variables in the regression analysis.
CRI-II (LDL-C/HDL-C ratio) represents the proportion or relationship between the atherogenic and antiatherogenic lipoproteins. CRI-II has been predictive power for cardiovascular disease [10]. CRI-II was a more precise predictor for cardiovascular events than classic lipid parameters (i.e., TC, TG and LDL-C) used independently [8, 31]. Katakami et al. [32] showed that CRI-II was useful in assessing the risk of early stage carotid atherosclerosis in type 2 diabetic patients. Fujihara et al. [33] demonstrated that CRI-II was an independent predictor of coronary artery stenosis and vulnerable coronary plaque. In a study involving 54 patients with CSF, Kalaycı et al. [34] reported that TG/HDL-C ratio, CRI-I and II values were higher in the CSF group than in the control group. The authors stated that age, smoking and TG predict CSF. In the present study, CRI-II was an independent predictor of CSF which was different than Kalaycı et al. [34] investigation.
CSF has been reported to be more common in young male smokers. In our study, both smoking and male sex were independent risk factors for CSF. These results are consistent with previous studies. In their cross sectional study, Sanghvi et al. [35] reported that history of tobacco use was 45.5% and male sex was 62.5% in the CSF group. Furthermore, current smoking was an independent risk factor for CSF. In another study performed by Rao V et al. [4] in an Indian population, 66% of patients were males and 68% of patients were smokers in subject with CSF. In a prospective study involving 39 patients with CSF, Arbel et al. [3] reported that current smoking was the most significant variable related to CSF. Smoking association with CSF could be explained as follows: endothelial dysfunction, impaired endothelium-dependent coronary vasodilatation, increased microvascular resistance, increased oxidized LDL, and increase in mediators leading to atherosclerosis [3, 5, 36, 37].
Study Limitations
This study had several limitations. First, this was a single-center, retrospective observational study with a small sample size. Because of its retrospective design, inflammatory markers related to atherosclerosis (e.g., high-sensitivity C-reactive protein, interleukin-6, and adhesion molecules) were not studied, and a more detailed evaluation of the relationship between CSF and inflammation could not be performed. Apolipoprotein B and small dense LDL-C, which reflect the total atherogenic particle load better than LDL-C, were also not measured. Unfortunately, imaging modalities (e.g., intravascular ultrasonography) could not be used, although these would have better demonstrated a potential relationship between CSF and subclinical diffuse atherosclerosis. In addition, selection bias may have occurred during selection of the control group due to the retrospective study design, and some individuals with NCF in the control group may have had undetected microvascular dysfunction.
{kind=link}