The COVID-19 pandemic has appeared as a daunting disaster for Bangladesh. With constrained resources and a gigantic population, the experience of Bangladesh illustrates some of the common challenges faced by the developing countries concerning the public health response to an infectious disease such as COVID-19. This article thus attempted to describe the scenario of public health preparedness and epidemiological characteristics of the first seven-months of the COVID-19 pandemic in Bangladesh.
Ineffective public health crisis communication and countermeasures
After the official announcement of COVID-19 cases in Dhaka, the Government took a number of initiatives to revamp the testing facility, medical equipment supply, and nationwide surveillance. The lockdown measures with the deployment of police and armed forces were routed to enforce the law. However, our study showed that public health countermeasures were not up to the mark to flatten the curve as the country was witnessing a steep rise in the number of confirmed cases. The human mobility data also confirms the gradual increase in mobility during the lockdown periods. A series of events such as the mobilization of 11 million mobile users from city to rural areas, local violence, massive gathering for Janaza prayer (funeral), and purposive rule-breaking indicated that people, by and large, failed to take into account the importance of maintaining social distancing. While strict lockdown policy has shown some success in China, New Zealand, Italy, and largely in the developed countries, a similar approach did not achieve the desired outcome in Bangladesh, for which the underlying socioeconomic and demographic factors were at fault. At the beginning of April during the lockdown period, Bangladesh had only 54 cases, but it increased to about 50,000 cases by the end of May as the lockdown ended. A similar trend was also observed in India and Pakistan where the early lockdown measures might have helped in the preparation of medical logistics but ultimately failed to contain the viral spread.
One recent study in Bangladesh has shown that people were confused about the "english" terms such as “stay at home,” “social distancing,” “quarantine,” and “lockdown” (19). The upward trajectory of positive cases despite an extended period of nationwide lockdown and restrictions indicate the inefficiency of public health risk communication. The gap in the public health preparedness in battling COVID-19 can be minimized by taking into account the nuances of geographical & cultural contexts and devising specific strategies. Significant investment and support are required to generate sufficient data for improving the efficiency of public health decisions.
Gender disparity and spatial distribution of infection
In Bangladesh, the proportion of men catching the virus was 2.5 times more than women, although studies around the world suggest that both men and women are equally susceptible to the virus (15,20). A similar observation was noted in India and Pakistan where men comprised about 65% and 70% of confirmed cases, respectively (21,22). This disparity in susceptibility might be due to cultural aspects since men dominate the outdoor activities and are less careful towards keeping up with personal hygiene. Also, the percentage of susceptibility might vary since COVID-19 is more fatal for men, causing them to seek medical care and subject to testing (23). The death rate among males was found higher in various studies around the world. In South Asia, males died in a higher proportion: India (64%), Pakistan (74%), and Bangladesh (77%). Studies showed that men over 60 years of age are twice as likely to die of COVID-19 than women (23,24). This could partly be explained by the presence of higher comorbidity and the smoking habit in men, although the exact reason remains to be elucidated (25). However, women in India had a higher case fatality rate compared to males (CFR: 2.9% versus 3.3%) which contrasts the scenario of Bangladesh (CFR: 1.4% versus 1.11%) (20,21). Future studies are warranted to understand the disparity in sex-specific mortality risk in South Asia.
In Bangladesh, the existing data suggest that the infection rate in people from urban areas is higher than in rural villages. This is unsurprising because urban settings offer a higher chance of catching the virus. For instance, the Dhaka or Chittagong city relies heavily on congested infrastructures where the population density is the highest, and the citizens receive reduced sunlight exposure. Vitamin D deficiency in city areas is well documented, and some early studies indicated that vitamin D deficiency could be a risk factor for COVID-19 adversity (26,27).
However, the rural remote regions of the country suffer from a lack of proper medical support. Out of 64 districts, almost half of the districts have over 100,000 people who are aged above 65 years, and data show that the proportion of the elderly is higher in rural areas (28,29). As hospital facilities and medical assistance are more centered towards urban residents, about 3 million people from 50 tribal and ethnic minor communities living in remote areas remain vulnerable to COVID-19 (28). In Brazil, around 9.1% of indigenous people infected with the disease died, and the rate of infection is soaring in distant communities (30). Correspondingly, the Rohingya refugee forcibly displaced from Myanmar are living in crowded quarters in Cox’s Bazar area, Bangladesh, where they are subject to several health issues such as malnutrition, limited medical access, food- and water-borne diseases, reproductive health, and communicable diseases. In addition to Bangladesh Government’s support, the UN initiative to mobilize women in spreading awareness regarding COVID-19 in Rohingya camps might lessen the disease burden; however, additional international aid is necessary to cope up with the challenges (31).
Low fatality rate as compared to other countries
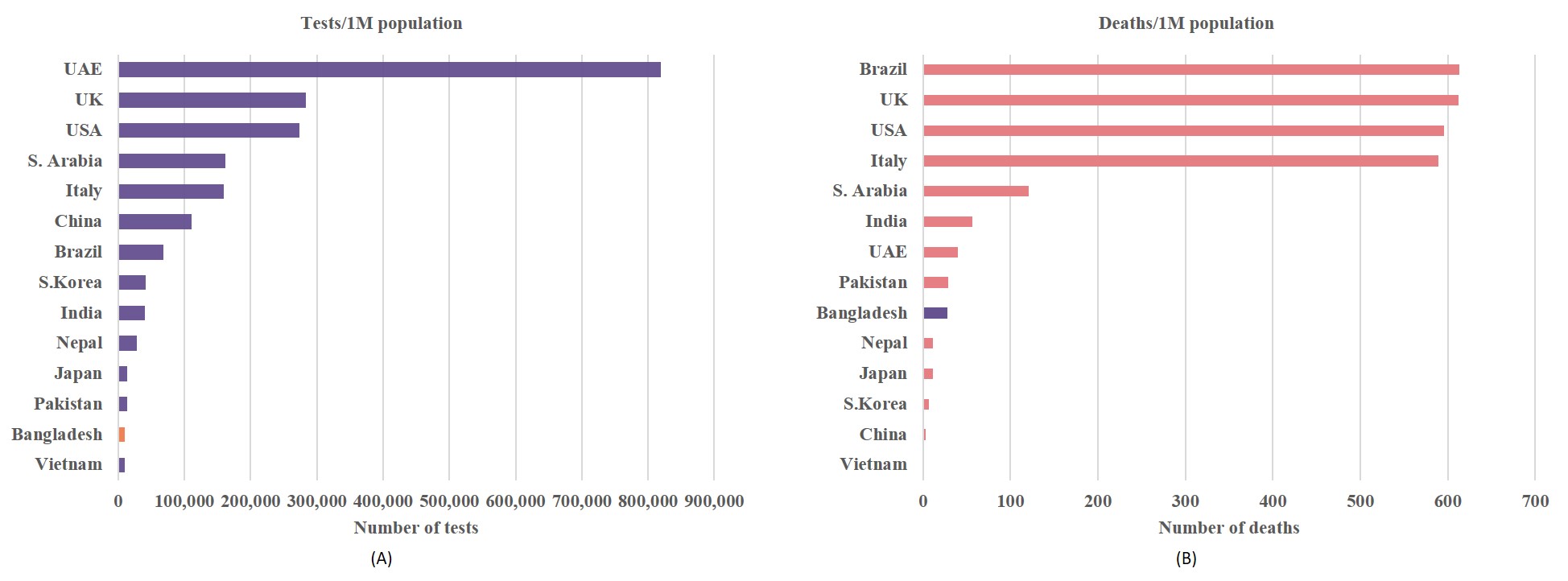
Interestingly, despite the official numbers jumping above 339,332 (as of 15 September 2020) cases, the death rate remained fairly low (1.4%) in Bangladesh and close to the other South Asian countries such as India (1.64%), and Pakistan (2.11%). This trend contrasts to the other countries such as Spain (4.88%), China (5.44%), France (7.36%), the UK (10.44%), Mexico (10.58%), and Italy (12.34%) (32). The lower mortality rate in the developing countries may be due to the fact that the overall life expectancy is within 64 to 72 years, leaving out the overly elder population; and there is a higher proportion of young populations in Pakistan, India, and Bangladesh. By comparison, the proportion of people aged over 70 years is much higher in the western settings (33).
Speculations regarding the low death rate in developing countries questioned the under-reporting of actual death cases as testing facilities were very limited. The unofficial sources indicated that a slightly higher number of deaths (n=2100) occurred in Bangladesh during the initial phase of the outbreak. However, the combined overall mortality rate remains surprisingly lower than what has been observed in the western world. The western countries offer care home facilities that are practically non-existent in South Asian culture where the extended family structure incorporates the elderly with the young in the same household. As opposed, the rapid spread of the infection among the elderly in care homes contributed to half of the total deaths in the western world. In France, the deaths linked to care homes were 51%, and in Canada, as many as 82% of COVID-19 deaths occurred among care home residents (34).
Slow progression of COVID-19 pandemic in South Asian countries
Despite higher population density and low awareness of personal hygiene, the South Asian countries have witnessed a rather noticeable slow progression. While Afghanistan and Pakistan's curves have flattened, India continues to see a sharp increase in the number of new infections. It is speculative that COVID-19 was already circulating in this region since South Asian countries are closer to and have strong economic relations with China. Of note, the first COVID-19 positive case was identified on January 30 in India, February 26 in Pakistan, and March 8 in Bangladesh. Despite such early detection, the subsequent numbers of infection and mortality continued to rise slowly. Several factors might influence the disease progression such as the wide-scale adaptation of facemask, tropical climate, or cross-immunity from other viruses as the region is under the high burden of disease (35,36). However, the most probable reason is that unlike China that locked down Wuhan city, the South Asian countries went for a nationwide total lockdown which slowed down the disease progression. Such actions had a tremendous impact on the daily lives of people, especially the daily wage earners and the measures turned out to be unsustainable. As the countries eased down on lockdown measures, the numbers began to soar up. In Bangladesh, a dramatic shift in the percent-change of disease transmission was observed as the post-lockdown COVID-19 infection was dispersing quickly from the cities towards the peripheral districts. This underpins the fact that relaxing social distancing measures might bring about similar infection rates for developing countries.
Overburden of healthcare system
A significant number of medical personnel and law enforcement workers were infected during the first wave of the COVID-19 epidemic. In particular, the fatality rate among the doctors in Bangladesh (3.16%) was higher than the healthcare workers in Pakistan (1.01%) and slightly lower than India (3.30%) and Afghanistan (3.75%) (37). The higher proportion of frontliners contracting the virus implies the lack of personal safety and inconsistency in management. The quality of personal protective equipment (PPE) and its training of proper handling remains in doubt. Moreover, hospitals suffer from the scarcity of intensive care units. With only 733 intensive care unit (ICU) beds in government hospitals, the healthcare has crumbled as the COVID-19 infection rate increases in torrent (38). It is surmised that the number of deaths in the age range of 60–70 could be subverted if proper ICU and medical support were provided. This underscores the need for urgent investment and remodeling of the healthcare sector.
Undoubtedly, the biggest problem with social distancing in Bangladesh lies in the population density and city-based centralized facilities. Besides, the healthcare system in Bangladesh is also largely centralized in metropolitan settings especially the capital Dhaka and divisional cities. The disaster of the COVID-19 pandemic thus points out the fragility of the existing system and urges to prioritize the decentralization of healthcare facilities. The steps can also ensure the minimization of the urban-rural disparity in the healthcare facilities. The establishment of universal health care should also be directed as a long-term goal.
Limited testing facility
The abrupt onset of critical patients at the hospitals has strained medical resources; and expensive PCR (polymerase chain reaction) based testing facilities and related workforce remained in pestilence to meet the demand. As shown in our results, the RT-PCR based test positive case rate has started to decline while the number of new deaths per day has remained largely unchanged, which could indicate that the current positive case rate is subject to the number of RT-PCR test performed. Since the laboratory test numbers have decreased, the incidence rate and the case rate may not be representative of the current situation of the COVID-19 pandemic. With regard to laboratory tests per million of population, Bangladesh is also lagging behind the race. Interestingly, the total number of tests performed by Japan (1,718,055) is fewer than Bangladesh (1,742,696), yet Japan has about 75,657 total cases as opposed to 339,332 cases in Bangladesh. This indicates that proper contact tracing and quarantining are equally important than simply performing massive tests.
Since public health measures in the developing countries are constrained by resources both in terms of financial support and trained workforce, it is essential to devise a strategy that is most suitable for such settings. It is recommended that instead of depending on RT-PCR based tests that are costly and time-consuming, the low-middle income countries could focus on syndromic diagnosis based on the constellation of symptoms and signs of COVID-19 in a disease afflicted area (39). This way, the burden of expensive testing could be largely reduced, the suspected patients identified earlier, and the investment channeled out into rebuilding healthcare facilities. Moreover, patients who were denied hospital admittance because of the absence of a COVID-19 test report will also receive early medical support. While the pandemic situation will not be under control very soon, the COVID-19 testing laboratories should be turned into regional surveillance centers instead of dissolving them by the time COVID-19 ends. Because only a national framework of proactive monitoring can assist in prompt action in the event of future outbreaks
Our study has a few limitations. First, we used publicly available recent data for analysis, which was both a weakness and a strength in itself. Second, unofficial death counts with COVID-19 like symptoms (not confirmed by the test) were extracted from well-established national news media and thus, these should be considered as probable death cases. Due to limited healthcare infrastructure and testing facilities, it was not possible to confirm all suspected deaths.
{kind=link}
{kind=link}