The lungs move up and down with breathing, especially the lower lung. Thus, the location of the pulmonary lesion is not fixed. Therefore, the position of the image marker during positioning may be different from the actual position after needle insertion. In addition, the lung is a loose air-containing organ with abundant internal blood vessels. In biopsy, a puncture needle is generally required to pass through normal lung tissue to reach the lesion. Pneumothorax, pulmonary hemorrhage or even air embolism may occur during repeated passages through the pleura and lung tissue. Based on these characteristics, needle biopsy for small pulmonary nodules (≤ 20 mm) is more difficult, and the probability of complications is increased.
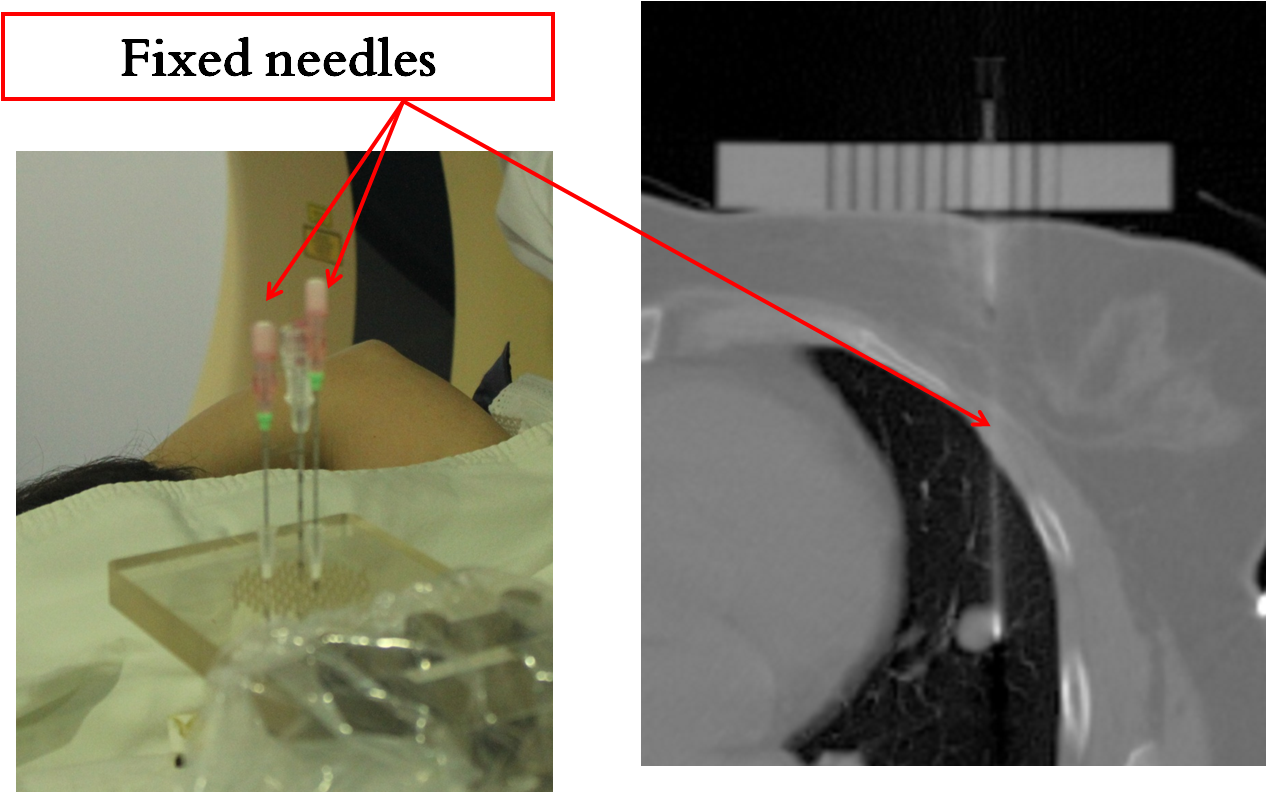
Since 2016, Chinese scholars have tried to apply 3D-printed coplanar puncture templates and fixed needle techniques to CT-guided percutaneous core needle biopsy of pulmonary nodules[11], but reports on this technology are rare. Therefore, we conducted a retrospective study to explore the clinical application value of 3D-printed coplanar puncture template-assisted CT-guided percutaneous core needle biopsy of small (≤ 20 mm) pulmonary nodules. In the present study, due to the different biopsy method, the accuracy of 3D-PCT-assisted CT-guided percutaneous CNB puncture was 95.2%, which was significantly higher than 85.8% in the Free-hand CNB group (p > 0.05). Many researchers have shown that compared with other puncture methods, CT-guided CNB has advantages in terms of accuracy or positive rates. For instance, Choi SH et al.[13] and Andrade JR et al.[14] reported an overall diagnostic accuracy of 95.0% and 92.3% during CT-guided percutaneous CNB of small pulmonary nodules (≤ 20 mm), respectively, and concluded that diagnostic accuracy is influenced by the biopsy method. CT-guided CNB is an excellent diagnostic tool, and its accuracy is high. Li Y et al.[15] reported an overall diagnostic accuracy of 93.5% during CT-guided percutaneous CNB of small (≤ 20 mm) pulmonary lesions. The diagnostic accuracy and yield of 3D-PCT group in the present study are slightly higher than those reported in the literature on CT-guided CNB.
Pneumothorax and pulmonary hemorrhage are the most common complications during percutaneous core needle biopsy of pulmonary lesions. The incidence of pneumothorax in the previous article was generally between 15% and 62%[6, 7, 16–20]. A previous study reported that risk factors for the development of biopsy-related pneumothorax include the presence of chronic obstructive pulmonary disease (COPD)[21], small lesion size[22, 23], a long needle path[22, 24], and technical factors, such as repeated pleural puncture[25] or a wider insertion angle of the needle[26]. We excluded COPD patients in our study, thereby avoiding patient-related risk factors for pneumothorax, and considered technical factors for pneumothorax. According to the present research results, because the patients in the 3D-PCT group used fixed needles while the control group did not use them, the number of repeated pleural punctures increased. This is an important reason why the incidence of pneumothorax in the 3D-PCT group was significantly higher than that in the Free-hand group.
According to reports, incidence of pulmonary hemorrhage ranges from 4–43% [7, 23, 24, 27], the present study revealed intrapulmonary hemorrhage rates of 49% (51/104) and 33% (35/106) for the two groups, respectively, and showed significant differences. The incidence of hemorrhage in Free-hand group is consistent with previous reports; however, in the 3D-PCT group it was more or less higher than previously reported. Scholars believe that repeated pleural puncture and greater lesion depth or long biopsy path are associated with an increased risk of bleeding [23, 24]. In present study, the use of fixed needles in the 3D-PCT group increased repeated pleural puncture, so compared to the free-hand group, the risk of hemorrhage increased. No complications of air embolism or tumor seeding of the pleura or chest wall were observed during percutaneous core needle biopsy of the pulmonary lesions.
Biopsy needle adjustments require CT scans to determine whether the angle and depth are adjusted correctly, so an increased number of CT scans was associated with an increased number of needle adjustments. With the assistance of a 3D-printed coplanar puncture template, the number of biopsy needle adjustments is significantly reduced, avoiding more iatrogenic radiation CT scans for patients.
The average surgical time in the 3D-PCT group was significantly greater than that in the Free-hand group, which was due to the increased time requirement for prepuncture preparation, including installation of the navigation system and 3D-PCT and fixed needle use, in the 3D-PCT group. The cost of surgery for each patient in the 3D-PCT group was 3590 Yuan equally, and that in the Free-hand group was 2100 Yuan, thus, 3D-PCT assisted percutaneous slightly increased the economic burden of patients.
The use of ROSE for triaging biopsy specimens has been encouraged by many scholars. For example, Collins et al. [28] showed that the ROSE service can improve cell block quality, thereby providing better utilization for IHC assessment and for IHC testing in positive diagnostic category cases. Fetzer et al. [29] concluded that ROSE can prioritize the management of tissue specimens to maximize tissue preservation and minimize waste. Nasuti JF et al.[30] demonstrated that ROSE can be beneficial in facilitating rapid clinical decisions and triaging specimens for ancillary studies. In our institution, ROSE is routinely used in CNB procedures. Interventional radiologists decide to rebiopsy based on the ROSE interpretation and triage the specimens, especially for preliminary diagnosis of malignant tumors or special infections (e.g., tuberculosis, Aspergillus, Cryptococcus neoformans) by ROSE. Based on our long-term practical experience, we believe that the application of ROSE for the triage of CNB biopsy specimens can prioritize the management of tissue materials for patients, minimize specimen storage, and play a role in precise diagnosis.
In conclusion, although 3D-PCT-assisted CT-guided percutaneous CNBs can increase the diagnostic rate, it will also bring more complications and increase the economic burden of patients. Therefore, whether 3D-printed Coplanar Puncture Template-assisted CT-guided percutaneous core needle biopsy of small (≤ 20 mm) pulmonary nodules should be clinically promoted requires comprehensive consideration.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}