Patient characteristics-
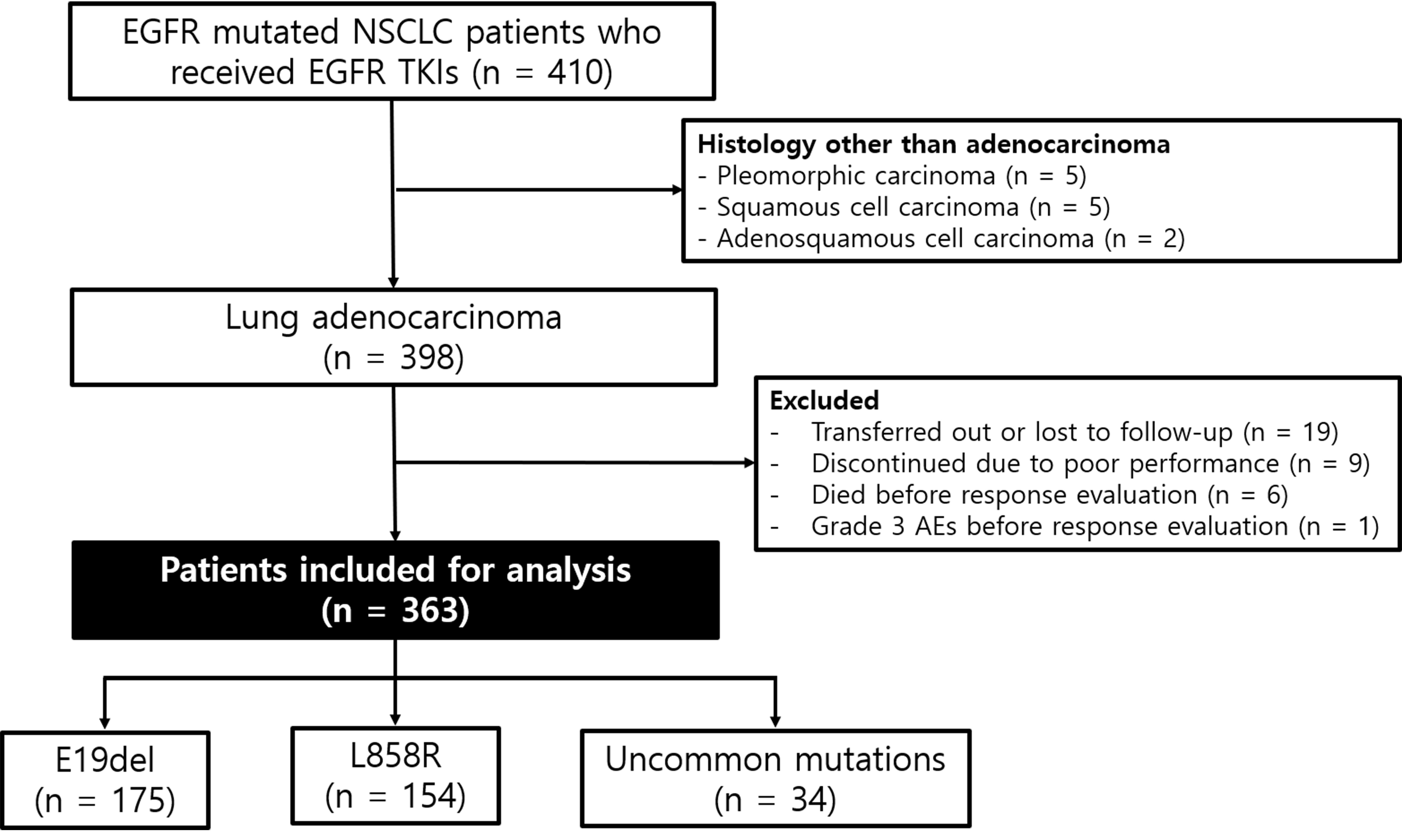
From May 2010 to December 2018, a total of 410 patients with advanced NSCLC underwent mutation testing for EGFR and received EGFR TKIs. Excluding 47 patients who met the exclusion criteria, 363 patients with advanced lung adenocarcinoma were finally included in the present study (Fig. 1). The mean age was 67.6 ± 11.0 years; 62.3% were females (Table 1). The frequency of E19del was 48.2%, that of L858R was 42.4%, and that of uncommon mutations was 9.4%. Of the 363 patients, 292 (80.4%) received EGFR TKIs as first-line treatment, and 10 (2.8%) received them as third-line treatment or beyond. No significant difference was found in treatment regimen among patients with each EGFR mutation type; afatinib was given to 102 (28.1%) patients, erlotinib to 139 (38.3%), and gefitinib to 122 (33.6%, p = 0.422).
Table 1
Baseline characteristics of the study population
| |
Total
|
E19del
|
L858R
|
Uncommon
|
p value
|
| |
(n = 363)
|
(n = 175)
|
(n = 154)
|
(n = 34)
|
|
|
Age, mean ± SD
|
67.6 ± 11.0
|
66.5 ± 11.8
|
69.1 ± 9.9
|
66.1 ± 10.8
|
0.076
|
|
Sex, male
|
137 (37.7)
|
68 (38.9)
|
59 (38.3)
|
10 (29.4)
|
0.572
|
|
BMI, kg/m2
|
24.0 ± 3.5
|
24.2 ± 3.6
|
23.6 ± 3.3
|
25.5 ± 4.0
|
0.012
|
|
Smoking status
|
|
|
|
|
0.691
|
|
Never smoker
|
258 (71.3)
|
123 (70.3)
|
109 (71.2)
|
26 (76.5)
|
|
|
Ex-smoker
|
76 (21.0)
|
36 (20.6)
|
35 (22.9)
|
5 (14.7)
|
|
|
Current smoker
|
28 (7.7)
|
16 (9.1)
|
9 (5.9)
|
3 (8.8)
|
|
|
Stage
|
|
|
|
|
0.361
|
|
Stage Ⅲ
|
31 (8.5)
|
15 (8.6)
|
11 (7.1)
|
5 (14.7)
|
|
|
Stage Ⅳ
|
332 (91.5)
|
160 (91.4)
|
143 (92.9)
|
29 (85.3)
|
|
|
Previous chemotherapy
|
|
|
|
0.442
|
|
0
|
292 (80.4)
|
137 (78.3)
|
126 (81.8)
|
29 (85.3)
|
|
|
1
|
61 (16.8)
|
34 (19.4)
|
24 (15.6)
|
3 (8.8)
|
|
|
≥ 2
|
10 (2.8)
|
4 (2.3)
|
4 (2.6)
|
2 (5.9)
|
|
|
EGFR TKIs
|
|
|
|
|
0.422
|
|
Afatinib
|
102 (28.1)
|
53 (30.3)
|
38 (24.7)
|
11 (32.4)
|
|
|
Erlotinib
|
139 (38.3)
|
69 (39.4)
|
61 (39.6)
|
9 (26.5)
|
|
|
Gefitinib
|
122 (33.6)
|
53 (30.3)
|
55 (35.7)
|
14 (41.2)
|
|
| Data are shown as n (%) per each group, unless otherwise noted |
| E19del, exon 19 deletion; L858R, L858R point mutation; Uncommon, uncommon mutations; SD, standard deviation; BMI, body mass index; EGFR, epidermal growth factor receptor; TKI, tyrosine kinase inhibitor |
Objective response rate
During a median follow-up duration of 24.9 months (range, 1.2–110.0 months), 209 patients (57.6%) died and 63 (17.4%) were still using EGFR TKIs at the time of data cutoff. The overall ORR and disease control rate (DCR) for EGFR TKIs was 73.3% and 93.1%, respectively (Table 2). ORRs were 76.0%, 76.0%, and 47.1% for E19del, L858R, and uncommon mutations, respectively (p < 0.001). However, no significant differences were found in ORR according to EGFR TKI regimen. In patients harboring E19del and L858R, no significant difference was found in ORR (Table 3). In patients harboring uncommon mutations, DCRs were 81.8%, 88.9%, and 57.1% in afatinib-, erlotinib-, and gefitinib-treated patients, although they did not reach statistical significance thresholds (p = 0.182).
Table 2
Response rate of epidermal growth factor receptor tyrosine kinase inhibitors according to mutation type and treatment regimen
| |
CR
|
PR
|
SD
|
PD
|
p value
|
|
Total (n = 363)
|
1 (0.3)
|
265 (73.0)
|
72 (19.8)
|
25 (6.9)
|
< 0.001
|
|
EGFR mutation types
|
|
|
|
|
|
|
E19del (n = 175)
|
1 (0.6)
|
132 (75.4)
|
33 (18.9)
|
9 (5.1)
|
|
|
L858R (n = 154)
|
0
|
117 (76.0)
|
30 (19.5)
|
7 (4.5)
|
|
|
Uncommon (n = 34)
|
0
|
16 (47.1)
|
9 (26.5)
|
9 (26.5)
|
|
|
EGFR TKIs
|
|
|
|
|
0.914
|
|
Afatinib (n = 102)
|
0
|
74 (72.5)
|
21 (20.6)
|
7 (6.9)
|
|
|
Erlotinib (n = 139)
|
1 (0.7)
|
100 (71.9)
|
29 (20.9)
|
9 (6.5)
|
|
|
Gefitinib (n = 122)
|
0
|
91 (74.6)
|
22 (18.0)
|
9 (7.4)
|
|
| Data are shown as n (%) per each group |
| CR, complete response; PR, partial response; SD, stable disease; PD, progressive disease; E19del, exon 19 deletion; L858R, L858R point mutation; Uncommon, uncommon mutations; EGFR, epidermal growth factor receptor; TKIs, tyrosine kinase inhibitors |
Table 3
Response rate of epidermal growth factor receptor tyrosine kinase inhibitors according to mutation type
| |
CR
|
PR
|
SD
|
PD
|
p value
|
|
Total (n = 363)
|
1 (0.3)
|
265 (73.0)
|
72 (19.8)
|
25 (6.9)
|
|
|
E19del (n = 175)
|
|
|
|
|
0.785
|
|
Afatinib (n = 53)
|
0
|
38 (71.7)
|
12 (22.6)
|
3 (5.7)
|
|
|
Erlotinib (n = 69)
|
1 (1.4)
|
54 (78.3)
|
10 (14.5)
|
4 (5.8)
|
|
|
Gefitinib (n = 53)
|
0
|
40 (75.5)
|
11 (20.8)
|
2 (3.8)
|
|
|
L858R (n = 154)
|
|
|
|
|
0.471
|
|
Afatinib (n = 38)
|
0
|
30 (78.9)
|
6 (15.8)
|
2 (5.3)
|
|
|
Erlotinib (n = 61)
|
0
|
42 (68.9)
|
15 (24.6)
|
4 (6.6)
|
|
|
Gefitinib (n = 55)
|
0
|
45 (81.8)
|
9 (16.4)
|
1 (1.8)
|
|
|
Uncommon (n = 34)
|
|
|
|
|
0.332
|
|
Afatinib (n = 11)
|
0
|
6 (54.5)
|
3 (27.3)
|
2 (18.2)
|
|
|
Erlotinib (n = 9)
|
0
|
4 (44.4)
|
4 (44.4)
|
1 (11..1)
|
|
|
Gefitinib (n = 14)
|
0
|
6 (42.9)
|
2 (14.3)
|
6 (42.9)
|
|
| Data are shown as n (%) per each group |
| CR, complete response; PR, partial response; SD, stable disease; PD, progressive disease; E19del, exon 19 deletion; L858R, L858R point mutation; Uncommon, uncommon mutations |
Survival outcomes
The median PFS of all patients was 12.1 months (95% confidence interval [CI], 10.2–14.0). A significant difference was found in the median PFS among E19del, L858R, and uncommon mutations: 14.7 months (95% CI, 12.6–16.8) for E19del, 10.9 months (95% CI, 9.0–12.7) for L858R, and 5.0 months (95% CI, 1.8–14.0) for uncommon mutations (p < 0.001; Fig. 2a). The median OS of all patients was 33.4 months (95% CI, 29.0–37.8) and a significant difference was found in the median OS among EGFR mutation types: 38.6 months (95% CI, 32.9–44.3) for E19del, 28.6 months (95% CI, 24.3–32.9) for L858R, and 22.8 months (95% CI, 18.2–27.4) for uncommon mutations (p = 0.001; Fig. 2b).
The median PFS times for afatinib, erlotinib, and gefitinib were 17.0 months (95% CI, 11.6–22.4), 11.2 months (95% CI, 8.9–13.5), and 10.9 months (95% CI, 8.3–13.5; p = 0.017; Fig. 2c). However, no significant difference was found in OS according to EGFR TKI regimen (Fig. 2d).
In patients harboring E19del, no significant differences were found in PFS and OS according to EGFR TKI regimen (Fig. 3a and 3b). In patients harboring L858R mutation, the median PFS times for afatinib, erlotinib, and gefitinib were 12.1 months (95% CI, 6.1–18.1), 9.2 months (95% CI, 5.6–12.7), and 10.9 months (95% CI, 7.8–13.9), respectively (p = 0.068; Fig. 3c). However, a significant difference was found in OS according to EGFR TKI regimen: 30.3 months (95% CI, 10.0–50.6) in afatinib-, 23.1 months (95% CI, 18.2–28.0) in erlotinib-, and 36.8 months (95% CI, 12.3–61.3) in gefitinib-treated patients (p = 0.031; Fig. 3d). In patients harboring uncommon mutations, a significant difference was found in the median PFS time according to EGFR TKI regimen: 12.1 months (95% CI, 0.0–25.6) in afatinib-, 8.2 months (95% CI, 7.0–9.5) in erlotinib-, and 3.0 months (95% CI, 1.4–4.5) in gefitinib-treated patients (p = 0.049, Fig. 3e). No significant difference was found in OS according to EGFR TKI regimen in patients harboring uncommon mutations (Fig. 3f).
Univariate analysis revealed that BMI, smoking status, EGFR mutation type, type of EGFR TKI, and line of treatment were associated with PFS. In multivariate analysis, BMI (hazard ratio [HR], 0.963; 95% CI, 0.932–0.994; P = 0.021) and EGFR mutation type (HR, 2.806; 95% CI, 1.850–4.255; P < 0.001) were associated with PFS (Additional file 2).
We evaluated isolated central nervous system (CNS) failure and bone failure without systemic disease progression during EGFR TKI treatment. No significant difference was found in the rate of isolated CNS failure among treatment regimen; however, patients who received erlotinib experienced significantly more isolated bone failure compared with those who received other regimens (18.7% in erlotinib versus 9.8% in afatinib and 9.0% in gefitinib, respectively, p = 0.036).
Serious adverse events
We evaluated the incidence of serious AEs which were defined as CTCAE grades 3 to 5. The overall incidence of serious AEs was 7.4%. The most common AEs were skin rash (5.0%), followed by gastrointestinal toxicity (2.2%) and myalgia (0.3%). The incidence of serious AEs was comparable among the three treatment groups. No treatment-related deaths occurred for all three drugs.
Acquired mutation after use of EGFR TKIs
Among 300 patients who discontinued EGFR TKIs at the time of data cutoff, 101 patients (33.7%) underwent re-biopsy for investigation of acquired resistance mutations. As a result, 50 cases (49.5%) acquired T790M mutation and one case transformed to small-cell lung cancer. Three cases (4.0%) were converted to EGFR wild-type (Table 4). No difference was found in the rate of acquired resistance mutations according to initial EGFR mutation type and treatment regimen.
Table 4
Acquired resistance mechanism after the use of epidermal growth factor receptor tyrosine kinase inhibitors according to mutation type and treatment regimen
| |
No change
|
T790M
|
SCLC
|
Wild-type
|
p value
|
|
Total (n = 101)
|
46 (45.5)
|
50 (49.5)
|
1 (1.0)
|
4 (4.0)
|
|
|
EGFR mutation types
|
|
|
|
|
|
|
E19del (n = 51)
|
21 (41.2)
|
27 (52.9)
|
0
|
3 (5.9)
|
0.447
|
|
L858R (n = 42)
|
19 (45.2)
|
21 (50.0)
|
1 (2.4)
|
1 (2.4)
|
0.601
|
|
Uncommon (n = 8)
|
6 (75.0)
|
2 (25.0)
|
0
|
0
|
0.371
|
|
EGFR TKIs
|
|
|
|
|
|
|
Afatinib (n = 38)
|
21 (55.3)
|
14 (36.8)
|
0
|
3 (7.9)
|
0.130
|
|
Erlotinib (n = 32)
|
12 (37.5)
|
19 (59.4)
|
1 (3.1)
|
0
|
0.168
|
|
Gefitinib (n = 31)
|
13 (41.9)
|
17 (54.8)
|
0
|
1 (3.2)
|
0.747
|
| A total of 101 patients underwent re-biopsy for investigation of acquired resistance after discontinuation of EGFR TKI. The most common mechanism was acquisition of T790M mutation, followed by conversion to EGFR wild-type, and transformation to small-cell lung cancer. No difference was found in the rate of acquired resistance mutations according to initial EGFR mutation type and treatment regimen. |
| Data are shown as n (%) per each group |
| SCLC, small-cell lung cancer; E19del, exon 19 deletion; L858R, L858R point mutation; Uncommon, uncommon mutations |
{kind=link}