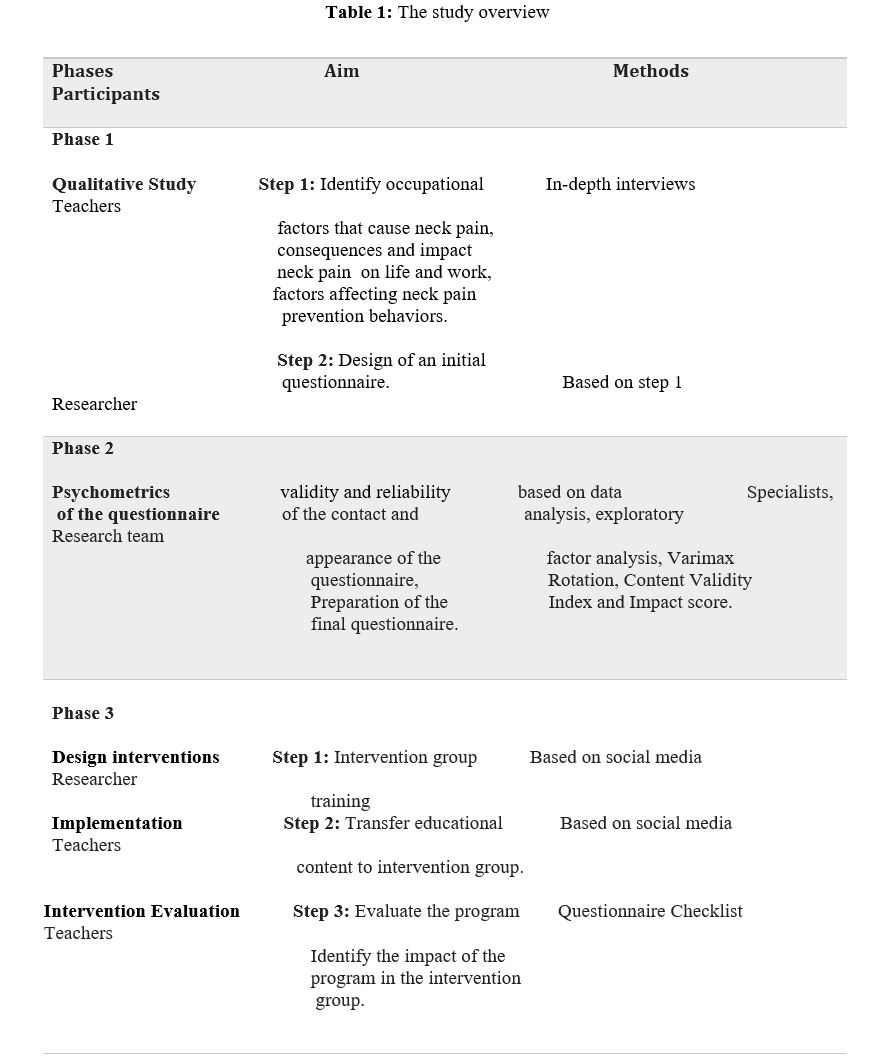
This study is a randomized controlled trial. The overall purpose is to study, develop and evaluate an intervention of model-based in social media to reduce job neck pain in school teachers. The study consists of three stages ( Table 1): The first phase of the research will be a qualitative study on 25 teachers. Criteria for entering this stage of the research: having a teaching job, having conscious satisfaction, having a job-related neck pain experience, willingness and ability to transfer experiences and diversity of research (education, gender, age, work experience). Data collection will be done through telephone calls and semi-structured interviews by the researcher with the participants. The questions will be designed based on the structures of the health belief model. Participants are asked questions about their experiences with job-related neck pain, its consequences and effects on work and life, the extent to which teachers suffer from neck pain, and the factors that affect neck pain prevention. Based on the analysis of the data obtained from the interview, items, sub-categories and main categories of the researcher-made questionnaire are prepared and compiled. The second stage of psychometrics is a researcher-made questionnaire. In this stage: the researcher-made questionnaire will be subject to content validity and face validity by 15 specialists in health education and health promotion, ergonomics, physiotherapy and occupational health. Exploratory factor analysis and scale correlation matrix will also be used to evaluate the construct validity and obtain the final items of the questionnaire. The third stage of the study includes: designing, developing and implementing an educational intervention based on the health belief model ( Fig. 2). At this stage, a list of all 26 schools in District 19 will be prepared. From schools, people are randomly selected and then randomly divided into two groups of intervention and control. The intervention group receives a training program while the control group does not receive any training program. Participants are evaluated in three stages of time: in the previous stage, one and three months after the intervention. The study environment will be public schools in the 19th district of Tehran province. Participants are junior high school teachers. Inclusion criteria in this study: Willingness to participate in study, access to the Internet and having the skills to use the Internet. Exclusion criteria include: unwillingness to continue to participate in research, having a second job, having congenital musculoskeletal disorders related to the neck, history of surgery, neck vertebral fractures and significant neck pain unrelated to the job, medical prohibition in Especially doing sports. The main purpose of this study is to prevent and reduce occupational neck pain in teachers, so we will identify the factors and behavioral factors that cause neck pain. And to promote neck pain prevention behaviors, we will design an educational intervention based on the Health Belief Model. The findings of this stage will be obtained through semi-structured interviews based on the Health Belief Model. Based on this, we can determine the factors affecting neck pain, the correction of which leads to change and continuity of behavior. These factors include: perceived sensitivity, perceived severity, perceived benefits, perceived barriers, Cues to action, and self-efficacy [31]. Based on the evaluation of the extent of each of these factors, it is possible to implement an intervention to change behavior. Educational content includes: definition of occupational neck pain and its causes, benefits of health behaviors, strategies to deal with barriers to neck pain prevention behaviors, improving self-efficacy in adopting and performing neck pain prevention behaviors, stressors in the workplace, the effect of stress On neck pain, stress management and control techniques, effective communication, anger management skills, excitement, ergonomic principles on neck pain prevention, corrective movements that reduce neck pain, stretching movements that strengthen neck muscles, how to sleep properly, how to Proper sitting and standing, correct posture when working with computer and telephone and doing daily chores. The educational content will be described based on evidence and using understandable language. Participants can communicate with the researcher by email and phone call. The intervention group will receive training in the form of webinars, group discussions, questions and answers, videos, animations, posters, pamphlets and infographics. How to receive training is supervised by the researcher. The trainings will be provided to the intervention group through social media for one month.
After that, reminder trainings will be provided to the intervention group for three months. During this period, the control group will not receive any intervention and after the intervention, the training package will be provided to the control group. The main outcome is the promotion of neck pain prevention behaviors that are assessed using a researcher-made questionnaire. Data collection instrument is a researcher-made questionnaire that is completed and collected in three stages, before, one and three months after the intervention. Questionnaires are completed anonymously to gain participants' trust in the intervention. The questionnaire based on the health belief model will have different domains (knowledge, perceived sensitivity, perceived severity, perceived barriers, perceived benefits, Cues to action, self-efficacy and behavior). Knowledge questions from the Likert three-part spectrum are true (2), no idea (1), wrong (0) and domain questions (perceived sensitivity and intensity, perceived barriers and benefits, self-efficacy and Cues to action) as spectrum 5 parts like, (completely agree 5), (agree 4), (no idea 3), (disagree 2) and (completely disagree 1) will be considered. Behavior questions are considered as a five-part Likert scale (never 1), (rarely 2), (sometimes 3), (often 4), (always 5). This questionnaire measures the variables of knowledge, attitude, perceived threat, self-efficacy, reinforcing factor and barriers to behavior and behavior. A higher score in each area of the questionnaire will indicate a better situation. This study will be conducted with power of 80% and 5% significance level. The sample size will be considered 10% drop,73 people are estimated for each group. In total, the number of participants in the study will be 146 people. For randomization, first a list of teachers' telephone numbers with a specific code is prepared and the codes are poured into a bag and randomly divided into two groups of intervention and control. This study is a double-blind study and the researcher and participants are not aware of it.
Statistical Analysis
The data obtained from the qualitative study will be analyzed based on Graneheim and Landman algorithms in qualitative content analysis. MAXQDA software will be used to encode semi-structured interview data. To evaluate the validity of the structure, factor analysis and scale correlation matrix and the Kaiser_ Meyer_ Olkin (KMO) Index and Bartlett's test sphericity will be used. The factor structure of the questionnaire is extracted using Varimax rotation. The quantitative data will be analyzed using SPSS V24. Descriptive statistics will include frequencies, means, and standard deviations. The Kolmogorov-Smirnov test will be used to check the normal distribution of data. Also, to compare the means between the two intervention and control groups of the test Independent-Samples T Test will be used. Paired t-test will be used to compare the means in each group at two points in time and ANOVA test will be used to compare the means in each group at three points in time. To analyze and evaluate the correlation between demographic variables, we will use correlation tests (Pearson for parametric data) and (Spearman or Kendall for non-parametric data) and Chi-square test.
{kind=link}