Study Design:
This was a randomized control trial. MASHS was implemented by a before-and-after intervention strategy which involved the random selection of the intervention and control groups obtained through cluster sampling such that for the intervention group, we used a unique SMS update portal named MASHS. This consisted of the main operator and the beneficiary who was in possession of a mobile phone. The operator generated the content of clear and understandable messages based on key variables of adolescent sexo-reproductive health.
Study Procedures:
To start the intervention, MASHS was introduced and explained to the families of participants. They expected three to five messages from the operator per week for a period of 6 months. Ethical and administrative considerations were highly considered. Using a 1:1 allocation concealment ratio, adolescent girls in Kumbo West Health District were randomized to receive a one-way text message on sexo-reproductive health or not. Figure 1 shows a flow chart of MASHS study design which was in accordance with the guidelines of the Standard Protocol Items: Recommendations for interventional Trials (SPIRIT).
Sample size determination:
The sample size calculation for this trial study will be based on sample size calculation for comparison between two groups 17as follows,
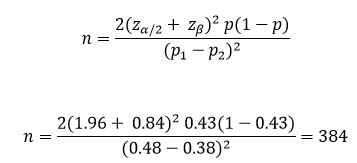
Zα/2=z0.05/2=1.96 (from z table or type 1 error of 5%)
zβ/2= z0.20=0.842 (from z table at 80%)
p1-p2=pooled prevalence=(prevalence in intervention group (p1) + prevalence in control group (p2)/2
n = 384
Considering non-response, we rounded up to n = 398.
Hence, 199 subjects for the control group and 199 subjects for the intervention group.
Sampling:
Multi-stage cluster sampling was used to select 6 health areas from the Kumbo West Health District (See Figure 2 showing the map of Kumbo West Health District-KWHD) namely BBH, Kikaikelaiki, Kitiwum, Kumbo_CMA, Kumbo_Urban and Melim in the Bui division of the North-West region of Cameroon and the participants were further selected using systematic random sampling from households. The various participants were then obtained via probability proportionate to size from the respective selected health areas.
Simple random allocation of Participants:
This was a parallel group design evaluating the effects of adding weekly one-way SMS messages using mobile phones to usual care (intervention) versus usual care alone (control) among adolescent girls. Eligible and consenting girls were then randomized to intervention and control arms using a 1:1 allocation concelament ratio by opaque sealed envelope method. A computer generated randomization list was generated using random block sizes of 2, 4 and 6 to prevent selection bias and enabled the production of the comparable groups for this trial. The allocation codes were then put in sequentially numbered opaque sealed envelopes and administered by the trained research staff at the office of KWHD services.
Training of interviewers:
The interviewers were trained using the adult learning theory for three days. These trained interviewers; blinded to group allocation, collected baseline data using a pretested data collection form containing socio-demographic data, sources of information on, and knowledge of reproductive health, knowledge and ever-use of contraceptive methods, knowledge of HIV/AIDS and sexually transmitted diseases, condom knowledge and attitudes, use and perceptions of health services at baseline and at 6 month intervals. The data analyst was also blinded to group allocation.
Trial Setting:
Cameroon is a culturally diverse coastal country in Africa, which lies on the western side of Africa on the Eastern Atlantic Ocean.18 Cameroon is bordered by Chad, Nigeria, the Central African Republic, Gabon, Equatorial Guinea, and the Republic of the Congo. The 2018 Cameroon population is estimated at 24.68 million.18 The study was conducted in Kumbo located in the North West region of Cameroon. The NorthWest Region is the third most populated region in Cameroon with Bamenda as capital.19 This study was precisely carried out in the Kumbo West Health District (KWHD), a semi-urban/rural community with many adolescent girls. BBH, Kumbo-Urban and Kumbo-CMA are semi-urban areas while Melim, Kitiwum and Kikaikelaiki are rural areas. The study involved community mobilization and participatory approaches which specifically were implemented in six randomly selected health areas of the KWHD. According to the Department of Economic and Social Affairs; Population Division of the United Nations, 12.3 and 10.5 percent20 of the total population make up the early adolescent girls (10-14 years) and late adolescent girls (15-19 years) population in Cameroon respectively. This gives a total of 22.8 percent adolescent girls of the total population of KWHD. Applying these population model we have a total of 25120 adolescent girls in the KWHD. The trial ran for six months, with outcome assessment at baseline and at 6 month intervals.
Participants: Inclusion/Exclusion criteria:
We included adolescent girls aged 10-19 years. We send the text messages to the adolescent girls or the parents/guardians of the adolescent girl that owned a mobile phone and could read text messages. Informed assent and consent was a prerequisite for participating in the study, and was provided orally and in writing. We excluded participants who refused to participate in the study and those aged less than 10 years or above 19 years.
Intervention: Mobile-based Adolescent Sexo-reproductive health scheme (MASHS):
We sent a one-way short text message to the participants in the intervention group in English. These messages were sent three to five times per week for a period of 6 months. We sent the messages at afternoon periods on Mondays, Wednesdays and Fridays between 4-6pm on those days. The content of the messages were motivating and acted both as a reminder and a cue to action (Figure 2: show an example of text messages used in the intervention phase). The message was sent through a phone number they could call back or text if they needed clarifications. The content was varied so as to retain participants' attention throughout the period of the study. The program secretary had a list of phone numbers to which he send the messages every week and used the 'delivery report' function to ensure that the messages had been delivered. The average cost for text messages on any networks in Cameroon is 50 CFA Frs.
Control:
In the control arm, subjects received the usual care provided to all adolescent girls as concerns sexo-reproductive health education which included education at schools and reproductive health services delivered at the health facilities of KWHD. They did not receive any text messages, but were interviewed at baseline and 6 months.
Administration of Questionnaires at before and after intervention:
A structured questionnaire was administered to selected adolescent girls who agreed to participate in the study. The questionnaires were interviewed-administered in English/Pidgin- English. The questionnaire was made up of four sections namely, i. Socio-Demographic Information, ii. Knowledge related questions on sexo-reproductive health iii. Attitude related questions on sexo-reproductive health and iv, Practice related questions on sexo-reproductive health.
Data management and analysis:
A coded number was given to identify each participant. Collected data was firstly entered into a research log book. Research questionnaires as well as work books and other study materials were stored safely in a locker in a safe location and secured by locking it with a lock. After collection of the data, the questionnaires were checked visually for completeness, obvious errors, and inconsistencies and then corrected. Data collected was entered daily into an electronic questionnaire (template) created in Epi info version 7 by the investigator. During the data entry process, 10% of data entered at the beginning was checked to ensure that the data was correctly entered. For confidentiality, the computer in which the data was stored was password protected and the information was accessible only to the researcher. Data was backed-up in an external hard drive and email box. The data was then imported into Microsoft excel spread sheet for cleaning/editing and finally analysed using social science package statistical software version 21. Descriptive and analytic statistics were performed.
Ethical Considerations:
The trial was conducted in compliance with the local protocol and applicable regulatory requirements in Cameroon. The study was approved by the Institutional Review Board of the Faculty of Health Sciences of the University of Buea (2018/193/UB/SG/IRB/FHS). Any deviations from the protocol were reported and explained. The study was conducted in accordance with the Helsinki declaration21 and other established clinical practice guidelines for research on human subjects. Research personnel approached all potentially eligible adolescent girls who fulfilled eligibility criteria for assent/consent. All adolescents’ girls signed a consent form or gave verbal consent to participate in the trial. Its Pan-African Clinical Trials Registry number is PACTR201805003259293