Main finding
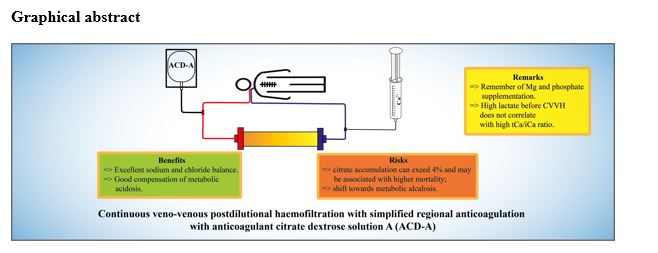
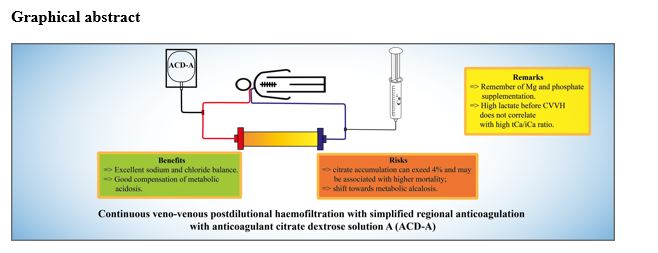
To the best of our knowledge, this is the first study to evaluate electrolytic homeostasis and metabolic control during the simplified ACD-A RCA protocol for CVVH on the Aquarius platform. In this prospective study, we found that CVVH with a simplified RCA protocol provides very good sodium and chloride balance, but it is related to significant incidences of magnesium and phosphate deficiency. We also found that the incidence of CA can be significant in cardiovascular surgery patients. Interestingly, the tCa/iCa ratio did not increase in many patients in whom CVVH was started at a high lactate level. Except for magnesium and phosphate, which should be supplemented during CVVH, the RCA protocol was found to be safe and associated with satisfactory ion and metabolic homeostasis.
Ionic concentration
When over 20 litres of body water per day is replaced with a substitution fluid, the problem of ion homeostasis must be addressed. It is possible that some ions are removed more easily than others during CRRT, and it is impossible to discuss CRRT safety without addressing the issue of ion balance. In our study, the serum potassium concentration was maintained within the normal range by the infusion of potassium chloride, and substitution solution bags were supplemented with potassium to reach 4 mEq/L. The investigation of the incidence of potassium abnormalities was not included in the aims of the study.
Sodium and chloride
Citrate, when administered as tri-sodium, can induce hypernatraemia [18]. However, previous studies on CVVHDF with RCA also reported a significant decrease in sodium levels after treatment, which was not observed in our group [12]. The use of ACD-A solution for RCA is related to a lower sodium load than the use of tri-sodium citrate-based RCA [5]. Therefore, with the ACD-A solution-based RCA protocol, low-sodium substitution fluid is not required to prevent a patient from developing hypernatraemia. The sodium concentration in the Accusol K0 used in this study was 140 mmol/L. The trend in the sodium level towards a narrow physiologic range led to decreased incidences of both hyper- and hyponatraemia within a short time after the initiation of CVVH RCA. The 2.4% incidence of hypernatraemia observed in our group during CRRT treatment was lower than that observed with protocols based on tri-sodium citrate solutions used for CVVHD [19]. The decreased incidence of hypo- and hypernatraemia and severe hyperchloraemia during the course of haemofiltration treatment observed in our patients indicate that the CVVH RCA protocol on the Aquarius platform is close to perfect with respect to sodium and chloride balance.
Calcium
In our study, the incidence of hypocalcaemia was higher than the results reported in previous studies on RCA for continuous veno-venous haemodialysis (CVVHD) and continuous veno-venous hemodiafiltration (CVVHDF) (2.8–13%), but this may have been due to the use of different diagnostic criteria [18, 20–23]. Khadzhynov et al. observed that during RCA haemodiafiltration, up to 66% of the measured iCa concentrations were outside of the normal range, leading to a 67.5% incidence of hypocalcaemia (< 1.1 mmol/L) [20]. The incidence of moderate hypocalcaemia (< 1 mmol/L) reported in his study (13.3%) was lower than that observed in our patients (18.9%) based on similar criteria [20]. He also reported severe hypocalcaemia (< 0.9 mmol/L) in three patients (20%), while in our group, we reported severe hypocalcaemia in 11 patients (22%), which was equal to 4.9% of all readings. Hypercalcaemia was observed more often before than during haemofiltration in the present cohort (4.9% of all readings during CVVH), and the incidence was higher than those previously reported from CVVHD and CVVHDF studies (2-2.5%) [19, 20]. The incidence of severe hypercalcaemia (0.7%) in our group was, however, lower than the 2% incidence observed by Khadzhynov [20].
The incidence of electrolyte imbalances is difficult to compare, not only due to different threshold values adopted for their identification but also due to the variance in reference values between laboratories and methods of analysis. According to our hospital laboratory, the normal range of iCa is from 0.98 to 1.21. A change in the calcium chloride concentration used for supplementation, which took place in our study protocol, should not have significantly influenced the results, as with initially lower concentrations, higher calcium chloride solution flows were used. Although the authors increased the target calcium range from the original RCA protocol, a substantial number of iCa readings were below the normal range, which indicates that the original protocol for the adjustment of calcium substitution was inadequate [14]. This might be of importance in cardiac surgery patients, in whom low iCa can exacerbate heart failure.
Magnesium
In addition to calcium, citrate chelates magnesium ions and moves them to the filtrate. This can lead to hypomagnesaemia if magnesium replenishment with the substitution fluid is not adequate. It was observed that post-filter magnesium concentrations decrease in a manner similar to the concentrations of calcium ions under RCA [24]. When using substitution fluid containing 0.5 mmol/L magnesium, a tendency towards a decreased magnesium concentration was observed during haemofiltration treatment. Magnesium is a very important intracellular ion that is responsible for crucial physiological functions. Prolonged CRRT with RCA can cause the depletion of its limited pool of approximately 1000 mmols. Despite routine magnesium sulfate supplementation at a rate of 0.81 mmol/hour, in our group, hypomagnesaemia was more common (22.3%) than previously reported from the CVVHD RCA study in cancer patients with AKI (2.3%) [19]. It was proposed that the magnesium concentration in substitution fluids used in ICU patients should be supra-normal rather than subnormal to compensate for increased losses due to its chelation by citrate [25]. Previously, supra-normal values of magnesium were observed in 54% of samples during haemodiafiltration treatment, which might increase the risk of muscle weakness [12]. In the studied patients, the magnesium level in the serum decreased over time during treatment with CVVH with A-CDA RCA. Significant hypomagnesaemia developed after 48 hours of CVVH.
Inorganic phosphate
The incidence of hypophosphataemia in ICU patients treated with CRRT without replacement solutions containing phosphate can reach up to 80% and is related to increased mortality [26]. The 34.4% incidence of hypophosphataemia in our study is comparable to other reported results when no-phosphate-containing substitution fluids were administered, but it is much higher than the 3% incidence reported in the study on CVVHDF with phosphate-containing fluids [27]. The observed increase in the incidence of hypophosphataemia over the course of CVVH treatment, although non-significant, could have deleterious effects on patient outcomes and should be corrected in future work to determine an optimal CVVH RCA protocol based on a phosphate-containing solution. The higher incidence of hypophosphataemia in survivors than in non-survivors might be attributed to their better general condition and lower need for parenteral nutrition. Phosphate was routinely intravenously supplemented in patients with parenteral nutrition, while it was administered only sporadically in patients who were fed enterally. As hyperphosphataemia mostly results from progressive renal dysfunction in AKI patients and could not be attributed to the CRRT protocol, the incidence of hyperphosphataemia was not assessed in this trial. The reported protocol might be improved by starting with higher supplementation doses of magnesium and inorganic phosphate than those used in the authors’ department.
pH and bicarbonate
During CRRT with RCA, acid-base status can be affected by excess citrate, leading to metabolic alkalosis or impaired clearance, which can result in an exacerbation of metabolic acidosis. Additionally, excess chloride could contribute to metabolic acidosis. The safe implementation of RCA requires a properly designed and flexible protocol with adjustable dosing. Strict adherence to such protocols should prevent metabolic impairment. The ACD-A solution used for RCA in our study has some advantages over the most commonly used tri-sodium citrate solution. Its use is related to the generation of 1/3 less bicarbonate after metabolism. A target citrate concentration in the filter compartment equal to 2.8 mmol/L should decrease the iCa concentration to 0.35 mmol/L on average [14] and provide effective anticoagulation [16]. According to the protocol, citrate flow was reduced stepwise when a trend towards alkalosis was observed, although this did not sufficiently counteract the development of metabolic alkalosis. The episodes of metabolic acidosis were most common at the beginning of CRRT therapy.
In the present study, the pH value and bicarbonate concentration increased significantly over time. Metabolic alkalosis during CRRT was more common in our study (25.2%) than in earlier studies on RCA for CVVHD: 14% observed in cancer patients [19] and 5% observed in ICU patients [20, 28]. However, this over-compensation of metabolic acidosis with the Aquarius CVVH RCA protocol might be beneficial in patients who are acidotic at the beginning of CRRT. A trend towards a higher pH and a higher bicarbonate concentration may indicate the presence of CA. It is a situation in which the capacity for citrate metabolism is not saturated and all citrate–calcium complexes are metabolized. The resulting net load of sodium leads to plasma alkalization by the increased strong ion difference, but an increase in the tCa/iCa ratio is not observed, and the iCa level remains normal.
In a previous study on CVVH with isosmotic citrate anticoagulation, Cassina et al. reported alkalosis (pH > 7.48) mostly of the respiratory type in only 4% of patients [11]. In contrast to our results, Khadzhynov et al. found that the bicarbonate concentration and base excess were below the normal ranges (69.9 and 84.6%, respectively) during RCA haemodiafiltration [12]. As also reported in previous studies, the results of our study indicated that most specific RCA protocols can cause upward or downward trends in bicarbonate concentrations and base excess. Jacobs et al. reported metabolic alkalosis (pH > 7.5) in 10% of patients treated with pre-dilution CVVH RCA in the group of patients treated with Prismocitrate 18 solution in contrast to its absence in patients treated with Prismocitrate 10/2 solution [29].
High anion gap metabolic acidosis (HAGMA)
HAGMA is frequently observed in conjunction with CA [5]. HAGMA and increased lactate concentrations are believed to appear not secondary to CA itself but rather to the shared primary problem of an impaired Krebs cycle, which reduces both citrate and lactate metabolism [5]. In our cohort, HAGMA was observed at less than 1.6% of all time points during haemofiltration, and it was lower during haemofiltration than at baseline. The low incidence reported in this study, despite the higher incidence of high anion gap, might result from trends towards a higher pH and a higher bicarbonate concentration.
Lactate
In our study, 23 haemofiltration sessions (10%) were started at a lactate concentration 4 mmol/L or above. However, it was observed that the risk of CA during RCA is low even in cases of severe hyperlactataemia and that lactate kinetics rather than concentrations should be considered in the assessment of the risk of CA [20]. In contrast to Tan et al., who found that hyperlactataemia predicted citrate intolerance, we did not find a correlation between lactate concentration before the initiation of RCA and the tCa/iCa ratio during haemofiltration treatment (Fig. 6) [13]. We postulate that rather than a single high lactate concentration, its increasing trend or even predicted lactate clearance after the initiation of CRRT should be considered when weighing the advantages and disadvantages of RCA in critical care patients.
Citrate accumulation
It has been suggested that each new CRRT RCA protocol should be assessed with respect to the incidence of CA and electrolytic disorders to enable clinicians to predict and possibly prevent potentially dangerous shifts and complications [12]. The measurement of the citrate concentration in the plasma is still not feasible or timely [22]. An increased tCa/iCa ratio is a reliable indicator of CA [5]. A tCa/iCa threshold of 2.5 is commonly used as an indication of CA; however, it has high specificity but low sensitivity as a risk factor for mortality [13, 30]. Some authors have proposed that this threshold should be decreased to 2.3, while others claim that it may be a poor indicator of ongoing accumulation [5, 30, 31].
Strategies have been developed to prevent CA. The citrate infusion rate can be significantly decreased from the initial dose. This must be accompanied by a decrease in the blood flow and the replacement fluid flow, rendering CRRT less effective, however theoretically without increasing the risk of filter clotting. An additional option is to continue up-titrating the calcium chloride infusion. Finally, if the ratio continues to increase, citrate anticoagulation can be replaced with systemic anticoagulation, or CRRT can be continued without anticoagulation [15].
Impaired citrate metabolism causes the build-up of calcium-citrate complexes, resulting in impaired free calcium recuperation. In fact, low iCa is the only known effect of citrate toxicity. Clinical symptoms in humans appear when the Ca++ concentration falls below 0.8 mmol/L. The first symptom is usually a prolonged QTc interval. With a further decrease in Ca++ levels, patients present with decreased cardiac contractility, hypotension, tremor, muscle weakness, coagulopathy, nausea and vomiting, and cardiac arrest [32]. In animal studies, the maximum citrate infusion rate without clinical symptoms was 0.67-1.00 mmol/kg/hour. In our study, the case of low iCa was observed in a patient with severe lactic acidosis, who should be excluded from citrate anticoagulation. In the studied patients, other indirect features of CA, such as escalating calcium requirements and the development of HAGMA, were rarely observed, making the diagnosis of citrate toxicity questionable. In the present study, the incidence of a high tCa/iCa ratio during haemofiltration treatment (4.6%) was higher than that observed during RCA for CVVHD, when it did not exceed 2.3 in any patient [19].
It is still a matter of debate whether RCA can be used in patients with high lactate levels before the initiation of CRRT. In our group, the median value of the lactate concentration did not increase, indicating that citrate anticoagulation did not inhibit lactate clearance, presumably due to adequate tissue perfusion in most of the patients. In our group, the 3.8% incidence of CA was slightly higher than the 2.3% reported by Khadzhynov et al. in a study with general ICU patients treated with CVVHD. However, in his study, patients with CA after over 48 hours of CRRT were excluded, so the entire incidence of CA was 3.8% [20]. The authors of this study concluded that the risk of CA during RCA is low even in cases of initial severe hyperlactataemia. During CVVH with RCA, the incidence of CA may be as high as 8–23%, depending on the CRRT dose [13, 33]. It should be emphasized that in our group, at three measurements, the tCa/iCa ratio was higher than 3.0, indicating a high risk of citrate toxicity. A tCa/iCa ratio up to 3.4 was previously reported in studies on RCA with high-dose haemofiltration (35–45 ml/kg/h) [13]. In our group, a higher incidence of CA was expected as a result of higher blood flows during CVVH, which require higher citrate doses than in most CVVHD protocols. Tan et al. observed citrate intolerance in 22.7% of patients treated with RCA haemofiltration [13]. Data from the literature on the incidence of CA in patients with hyperlactataemia treated with RCA CRRT are limited, and questions arise regarding whether refusing these patients the benefits of RCA is reasonable [20]. Our study is not exceptional in the fact that RCA CRRT was started in patients with hyperlactataemia. In a previously described group of 1049 patients, CRRT was started in 221 ICU patients with lactate levels exceeding 4 mmol/L, in whom the reported incidence of CA was 6.3% [20].
{kind=link}
{kind=link}