In this study, the clinical procedures for spasticity assessment were visually analyzed using an electrogoniometer (Experiment 1). Additionally, a preliminary validation of the measurement device developed according to the results of Experiment 1 and a comparison of measurement conditions were conducted (Experiment 2), which indicated that an angular velocity of 300°/s was the best in detecting spasticity. Subsequently, the validity and reliability of measurement with the determined condition were tested using a larger sample size in Experiment 3, which showed high test–retest reliability and concurrent validity with MAS. The measurement at an angular velocity of 300°/s significantly correlated with MAS (r = 0.84, P < 0.01) and detected the difference between the control group and MAS1 subgroup, as well as the MAS1 and 2 subgroups.
The results of Experiment 1 indicated that in the clinical evaluation of spasticity, the clinicians moved the patients’ ankle at an angular velocity of 268 ± 77°/s. This was faster than the velocities employed in previous studies on the mechanical measurement of spasticity, which ranged from 25°/s to 211°/s [4, 15, 19, 20, 31]. As reported by previous studies, spastic responses to passive joint movement are velocity-dependent [20, 32]. Thus, the fast velocity employed by clinicians may contribute to an increase in sensitivity in detecting spasticity. The necessity of this fast angular velocity was further tested in Experiment 2 using a measurement device developed based on observations of the clinical maneuver. Among the velocities of 100°/s, 150°/s, and 300°/s, 300°/s was found to best discriminate the patient group from the control group and to also best differentiate between different degrees of spasticity classified using the MAS score. Altogether, these results strongly support the importance of angular velocity in improving the sensitivity of the mechanical measurement of spasticity.
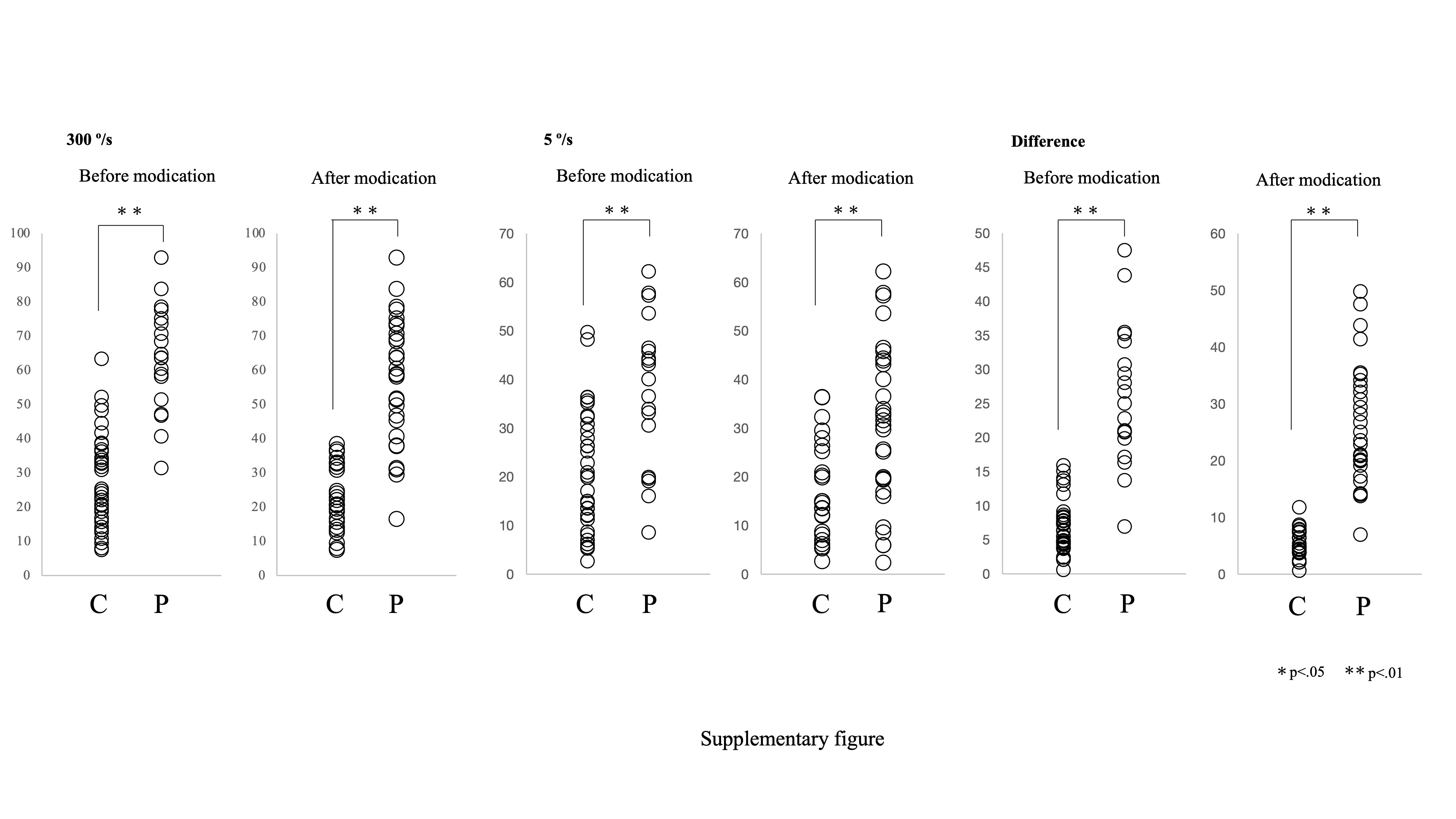
In addition, the video analysis of the measurement procedure in Experiment 1 revealed the small tips that could possibly affect the accuracy of the measurement. For example, the clinicians often added a preparatory slow stretching movement prior to the rapid dorsiflexion of the angle for the measurement. This might have potentially affected the sensitivity of the measurement of velocity-dependent spasticity, as the elastic component of ankle resistance, which can be reduced by passive stretching [33, 34], influences the measurement of resistance force. Our preliminary evaluation support the utility of these clinical-maneuver based modifications; the difference in measurement values between the patients and the healthy subjects was clearer with these modifications than without them (supplementary Fig. 1). The necessity of each of these additional tips in the measurement of spasticity should be further clarified; nonetheless, these results may support the potential benefits of this clinical practice-based approach in the development of methodology for mechanical measurement.
In Experiment 3, the validity of the measurement at an angular velocity of 300°/s was further tested using a larger sample size. The results indicated that the differences between the subgroups could be detected with this measurement condition; the differences between the control group and MAS 1 subgroup, as well as the MAS 1 and 2 subgroups, were significant. These results support the sensitivity of this measurement methodology at a high angular velocity of 300°/s in detecting the differences in spasticity. Previous studies showed the validity of the mechanical measurement of spasticity in joints such as the ankle and wrist joints, with a significant correlation with clinical scales such as MAS or MTS [22, 32]. However, the strength of correlations with clinical scales and the discriminative capacity to differentiate the extent of spasticity were still limited. In this study, we reported a high correlation between the measurement values and MAS score (rs = 0.84) and the detection of the existence of mild spasticity (MAS 1) and difference in mild and moderate spasticity (MAS1 and 2). These results may improve the clinical feasibility of the measurement methodology developed in this study.
In contrast, no significant differences in the measurement at a velocity of 5°/s were identified between the MAS subgroups. As the low angular velocity of 5°/s was insufficient to induce a stretch reflex response [19, 35], measurements at 5°/s would reflect the resistance to movement due to non-neural factors such as the elastic properties of muscles and connective tissues [36]. Therefore, the comparison between fast and slow conditions is considered to mainly reflect the neural component of spasticity [37].
The results obtained in this study may further contribute to the detailed understanding about spasticity. There have already been several attempts to separate the neural and non-neural components of spasticity in previous studies [15, 37–39] that were based on biomechanical modeling, using mechanical measurement under several different velocity conditions. In this study, we succeeded in discriminating different degrees of spasticity via a simple measurement with mechanically controlled passive ankle movement at fast and slow velocities, without conducting a sophisticated component analysis with biomechanical modeling. Further combination of this measurement methodology with biomechanical modeling may further improve the accuracy of the estimation of neural and non-neural components of spasticity, promoting a more detailed understanding about the mechanism of spasticity.
Study limitations
This study has some limitations that should be considered. First, the analysis of the clinical maneuver was performed in a single hospital with a limited number of clinicians; thus, the findings cannot be generalized as a common maneuver used by clinicians. However, considering the high discriminative capacity achieved in this study, clues to improve the accuracy of the mechanical measurement of spasticity were at least provided. Second, an electromyographic analysis was lacking, which would have confirmed the presence or absence of a stretch reflex response during maneuvers, thereby supporting the analysis of the contribution of the velocity-dependent component of joint resistance. Our study focused on the relationship between the speed of joint movement and the resistance force. Future studies combining torque measurement with this methodology and electromyography would aid in further understanding the mechanism of the response against joint movement. Third, due to technical limitations, we could not test at a higher velocity than 300°/s. Therefore, it is possible that a higher velocity better distinguishes spasticity. Further technical development may facilitate the understanding of the velocity-response relationship in the measurement of spasticity.
{kind=link}