This is the first randomized, double-blind, parallel group, controlled trial that directly compared the rehabilitative effect of sequential 4-channel NMES with conventional 2-channel NMES. In the present study, clinical improvement was observed via sequential 4-channel NMES and 2-channel NMES in VDS. Only the sequential 4-channel NMES group showed significant improvement in PAS, FOIS, and subset of MDADI (functional) after treatment. When we directly compared the improvement between the two groups, the 4-channel group was superior to the 2-channel group in oral and total VDS.
PAS improvement in sequential 4-channel NMES is a very important finding. Previous studies on 2-channel NMES showed conflicting results. Some studies have proven effectiveness, [23, 24] but others have shown no effect.[8, 25] The reason might depend on the application site and methods of NMES. In a previous study, NMES on submental placement alone does not change the PAS and National Institutes of Health-swallowing safety scale (NIH-SSS). However, submental and throat placements show a significant improvement in the NIH-SSS, but PAS is unchanged.[9] Two-channel NMES improves pharyngeal peristalsis and cricopharyngeal functions at the esophageal entry but does not affect the elevation of the hyolaryngeal complex, which has correlation with aspiration or penetration.[9, 13]
In a previous study that used 4-channel NMES by connecting two sets of 2-channel NMES suggested that the sequential 4-channel NMES facilitates the movement of hyolaryngeal structures during swallowing.[17] However, this system was made by combining two sets of 2-channel NMES; therefore, we could not adjust each channel. Thereby, we activated the first two channels for 1400 ms, then 300 ms later, and the third and fourth channels were activated for 1100 ms. The biggest difference from the previous study is that we stimulated the third channel, which is attached to the thyrohyoid muscle in 150 ms after stimulation of the first and second channels. A previous study evaluated during the effect, but the present study evaluated rehabilitative effect, which is commonly used for conventional 2-channel NMES.
The stimulation algorithm of sequential 4-channel NMES is based on normal contractile sequence. In the EMG analysis, the activations of the suprahyoid muscles developed about 150 ms and 350 ms earlier than those of the thyrohyoid and other infrahyoid muscles (sternohyoid and sternohyoid muscles). After 1400 ms of suprahyoid muscles’ contraction, all of these muscles stop their contractions simultaneously.[10] These sequential contractions of the suprahyoid and infrahyoid muscles accomplish the circular motion of the hyoid bone. The thyroid muscle assists laryngeal elevation, and other infrahyoid muscles, such as sternohyoid, sternothyroid, and omohyoid muscles, assist in prolonged laryngeal elevation and upper esophageal sphincter opening.[10, 26] This concept was verified by using kinematic and pressure analyses in a previous study.[17] Thus, the contractions of the thyrohyoid and other infrahyoid muscles, which have proper interval time with those of the suprahyoid muscles, may be important for dysphagia treatment, and our results verified the improvement of laryngeal complex for aspiration or penetration.[10]
The only muscle that elevates the larynx to the hyoid is the thyrohyoid muscle, which lies beneath the strap muscles, such as sternohyoid, sternothyroid, and omohyoid muscles.[9] In 2-channel NMES, simultaneous stimulation of submental and throat regions showed hyolaryngeal descent because sternohyoid and omohyoid stimulations exceeded the hyolaryngeal elevation effects. In other words, electrodes over the anterior neck might activate the sternohyoid and omohyoid rather than thyrohyoid and suprahyoid muscles. This hyolaryngeal descent is not a physiologic motion; therefore, the main mechanism of 2-channel NMES is strengthening of swallowing-related muscles.[27] However, theoretically, as 4-channel NMES uses normal contractile algorithm, the main mechanism of 4-channel NMES is not only strengthening of the supra and infrahyoid muscles but also increasing coordination of swallowing-related muscles.
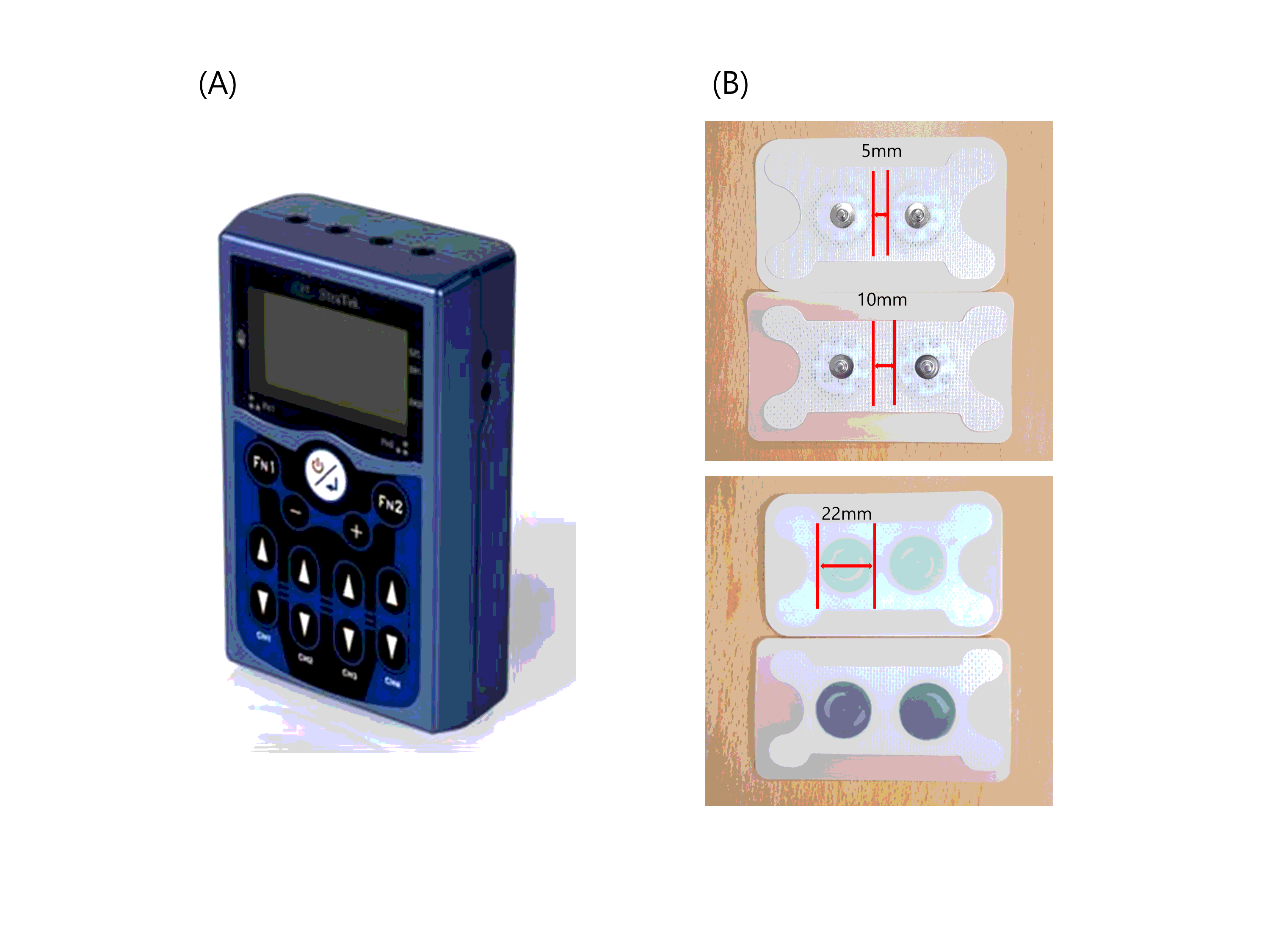
In the present study, oral VDS and total VDS were significantly improved in the 4-channel NMES group compared with the 2-channel NMES group. Tongue-based pressure has been previously turned out to be important when the tongue comes in contact with the posterior pharyngeal wall, squeezing out the bolus through the pharynx.[28] Alterations in tongue coordination, strength, and pressure generation may result in a disruption of bolus movement from the oral cavity to the pharynx and result in increased risk of aspiration before or after swallowing.[29] Also, a previous study showed that a greater tongue strength results in a greater activation of the suprahyoid muscle during swallowing.[30] In the present study, one channel was attached to the suprahyoid muscles in 2-channel NMES, and the first and second channels were attached to the bilateral suprahyoid muscles in 4-channel NMES. Considering that the effective depth of NMES is directly proportional to the distance between stimulation electrodes,[31] a wider placement of the coupled electrodes might more effectively stimulate not only the suprahyoid muscles but also the genioglossus or tongue muscles. Therefore, more channels and more covered lesion of the suprahyoid lesion in the sequential 4-channel NMES seem to induce effective contraction of the genioglossus and tongue muscles, which is highly correlated with tongue motion and is able to improve the strength of the tongue base, thereby resulting in superior efficacy in oral VDS scores.
In the present study, one participant in 2-channel NMES dropped out due to discomfort during NMES. In the 4-channel NMES group, aggravated dizziness was not related to NMES; therefore, no complication was developed. As sequential 4-channel NMES stimulated swallowing-related muscles with normal contractile algorithm, thereby inducing physiologic motion, less discomfort developed. Although the sample size was small and complication rate was negligible, 4-channel NMES is a safe and well-tolerated treatment method for dysphagia.
Originally, the purpose was to calculate the number of subjects in a future clinical trial to confirm the superiority of 4-channel NMES for future clinical trials. However, as 4-channel NMES sequentially stimulates swallowing-related muscles functionally and uses multi-channel for strengthening effect, our study verified the superiority of 4-channel NMES to 2-channel NMES with a small sample size. Follow-up study to verify the effectiveness of 4-channel NMES for pharyngeal phase is required.
This study has some limitations. First, a small number of subjects were included as this trial was a pilot study. As a result, pharyngeal VDS and FOIS were not significantly different between the two groups. However, the small number was enough to prove the superiority of 4-channel NMES in oral and total VDS. A follow-up study is required to verify the significant improvement of pharyngeal VDS and FOIS. Second, treatment duration and daily sessions were different among the 5 rehabilitation units and general patients’ condition. To manage this limitation, we did not use treatment frequency and time for the amount of NMES treatment, but used 420 min and 840 min as minimal and maximal treatment durations, respectively.
{kind=link}