Search results and included studies
After excluding duplicate articles, we had 1532 potentially relevant records based on the search strategy and additional manual search. During subsequent review, 13 studies that met the inclusion criteria were further evaluated for eligibility, and five full-text articles from 1995 to 2015 were included in this meta-analysis (12, 14, 19, 25, 26). The review process is illustrated using a flowchart of Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (27) (Figure 1).
Baseline characteristics of included studies
All five included studies were prospective, randomized controlled trials with a total of 423 patients (84.8% men); the weighted-average age was 51.1 years, and 34%–55% of the patients had alcoholic cirrhosis; in addition, a substantial portion of the patients were classified as Child–Pugh class B (39%–47%) or class C (24%–55%). Typical included patients exhibited cirrhosis with the first attack of acute esophageal variceal bleeding. Those who did not exhibit cirrhosis, exhibited hepatocellular carcinoma or portal vein thrombosis, or those who had previous variceal bleeding were generally excluded from these studies (12, 14, 19, 25, 26). The baseline characteristics of patients are summarized in Table 1 and Table S1, and they were similar between the EVL and standard combination groups.
After the index bleeding episodes, endoscopic treatments were performed within 6 to 24 hours; and the three conducted studies after 2000 involved the use of multiband ligators for hemostasis (12, 14, 19). The rate of active spurting during the index endoscopy was similar in both groups (32% vs. 36% in EVL vs. standard combination group, p = 0.246). Vasoconstrictors, including terlipressin, octreotide, and somatostatin, were prescribed either before (25) or after emergency endoscopy (12, 14, 19, 26). The dosages were in accordance with the recommendation of current international guidelines (1, 7), except for the study by Peng (19) in which terlipressin was prescribed at a dose of 1 mg QD. In the control group that did not receive vasoconstrictors, proton pump inhibitor (12), propranolol (19), and placebo (14) were prescribed as concomitant medical therapy.
Risk of bias assessment
Risk of bias in each randomized clinical trial was evaluated using the Cochrane Collaboration’s risk of bias assessment tool; the results are summarized in Table S2. Among these studies, only one had a double-blind design (14) and one was a single-blind study with respect to the examiner only (12). All studies generally had a ratio of 1:1 for randomization of participants; however, none of the studies described the detailed randomization and allocation concealment procedure.
Primary outcomes: initial hemostasis and rebleeding, treatment failure, and mortality in the first 5 days
The numbers of patients with major outcomes in each study are summarized in Table 2. Rate of initial hemostasis was reported in all articles, with the range from 93%–100%, and the pooled estimate were almost the same between the EVL or standard combination groups (97.6% vs. 98.0%, RR = 1.00, 95% CI = 0.97–1.02, Figure 2a).
Five-day rebleeding rates were also available in all the included studies, and most of them exhibited a nonsignificant RR during the meta-analysis except for the study by Sung et al. (25), which favored combination therapy. Although a trend toward higher rebleeding rates in the EVL group was observed, the pooled estimate was not statistically significant (15.9% vs. 6.6%, RR = 2.25, 95% CI = 0.87–5.77, p = 0.09, Figure 2b).
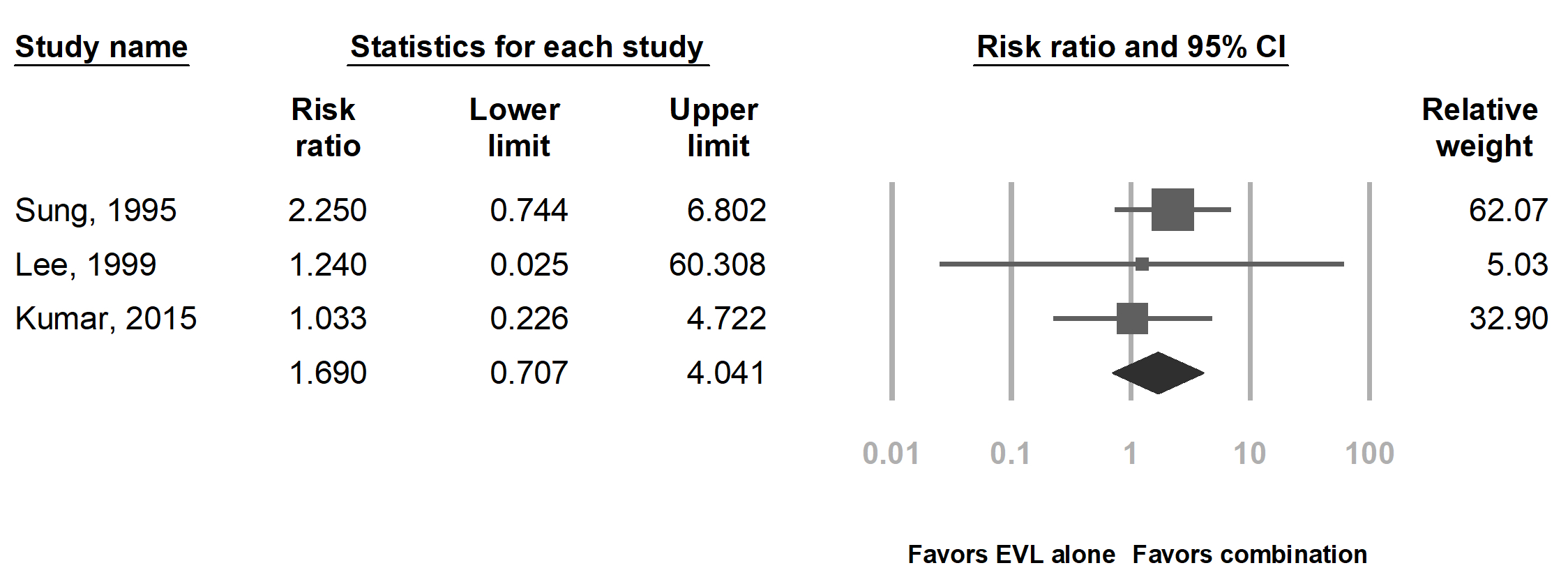
Mortality rate was presented as death within the first 5 days (12, 19, 26) and in-hospital mortality (14, 25, 26). The meta-analysis did not reveal a significant difference in 5-day rebleeding rates (0 vs. 0.7%, RR = 0.81, 95% CI = 0.09–6.87, Figure 2c) or in-hospital mortality rates (11.2% vs. 6.8%, RR = 1.69, 95% CI = 0.70–4.04, Figure S1) between the groups. Treatment failure within 5 days was documented in all studies except for the study by Sung et al. (25). The pooled result showed that similar results were obtained using EVL alone and standard combination therapy (9.6% vs. 6.7%, RR = 1.43, 95% CI = 0.54–3.75, Figure 2d).
Secondary endpoints: 6-week mortality, adverse events, hospital stay, and transfusion requirement
Six-week mortality was documented in three studies (12, 19, 26). With meta-analysis, the 6-week mortality was similar between the EVL and standard combination groups (2.9% vs. 3.0%, RR = 0.88, 95% CI = 0.25–3.13, Figure 3). Adverse events of both groups were reported in three studies. In the study by Lee et al (26), cases of aspiration pneumonia (two and three in the EVL and standard combination groups, respectively) and one case of spontaneous bacterial peritonitis in the standard combination group were observed during hospitalization. By contrast, the study by Lo et al. reported a significantly larger number of patients with chest pain and abdominal pain in the standard combination group than in the EVL group (22/60 vs. 0/60, p < 0.001) (12).
The length of hospital stay was also reported in two studies. Lee et al. (26) suggested significantly longer hospitalization in the EVL group than in the standard combination group (16 ± 11 vs. 11 ± 4 days, p = 0.028), whereas Lo et al. (12) did not report any difference between the groups (8.8 ± 3.8 vs. 9.4 ± 2.3 days, p = 0.45). In addition, the duration of intensive care unit stay was similar in both the groups (14, 26). In terms of transfusion requirements, the need for transfusion in the standard combination and EVL groups was similar (14, 19, 25, 26); however, the different parameters reported in each article precluded further meta-analysis.
Sensitivity analysis and evaluation of publication bias
Sensitivity analysis by excluding one study at a time was undertaken for meta-analysis of the primary outcomes. For initial hemostasis, 5-day mortality rates, and treatment failure, the pooled estimate did not exhibit significant changes during analysis. By contrast, significantly higher 5-day rebleeding rates were observed with EVL alone (14.7% vs. 2.7%, RR = 4.02, 95% CI = 1.76–9.20, Figure 4a) when the study of Kumar et al. (14) was excluded than when it was included; furthermore, cumulative analysis revealed that the pooled estimate favored the standard combination group until this study was included (Figure 4b). Excluding any other study did not result in significant changes from the initial meta-analysis. However, the difference in rebleeding rates was considerably smaller (9.6% vs. 6.1%, RR = 1.26, 95% CI = 0.59 - 2.69) if the study by Sung et al. (25) was exluded, which was the only study showing significantly higher rebleeding in the EVL than in the standard group in this review.
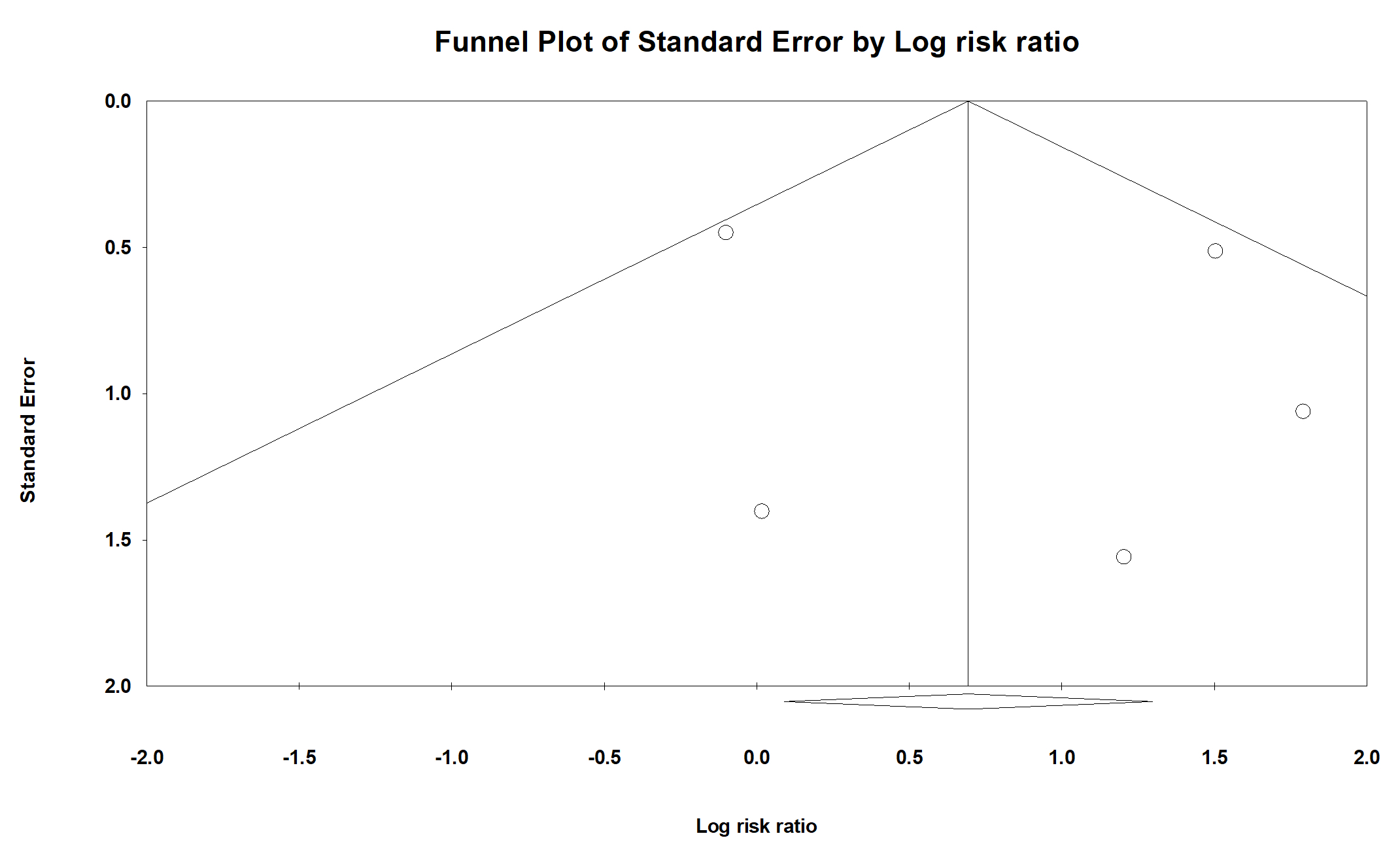
Publication bias was assessed using pooled estimates of 5-day rebleeding (Figure 4c). Obvious bias was not observed on the funnel plot and Egger’s test did not provide significant results (one-tailed p = 0.337).
{kind=link}
{kind=link}