Program implementation
Program description: AIM process.
The goal of the AIM process (Assess, Identify, Make it happen) is to implement evidence-based practices (EBPs) for promoting student nutrition and physical activity in school settings. For each school participating in AIM, a task force of community stakeholders (including the school principal, classroom teachers, physical education teachers, school staff, food service directors, nurses, parents) convenes for a series of meetings led by a facilitator trained and certified in the process. The AIM facilitator is provided a ‘facilitator guide’ which includes detailed agendas, activities, and talking points for each meeting in the process, as well as actions and tasks to complete between the meetings. Before the AIM process begins, baseline data is collected via a three-module survey based on the School Environment and Policy Survey (SEPS) (Author et al., 2013). This survey is completed by the principal, food service director, and physical education teacher and generates a Best Practice Report that provides the status (fully implemented, partially implemented, not implemented) of EBPs for nutrition and physical activity.
After the task force has been recruited and oriented to the process, they discuss strengths and challenges related to student health behaviors and school practices to promote student health. The task force also reviews the Best Practice Report to understand the current implementation status of nutrition and physical activity EBPs in the school and generate a list of potential changes to make to the school. This list of potential changes is later revised and clarified before final selections are made based on the importance of a change for student health and the feasibility of implementing it.
The task force engages in several action planning activities to promote the successful implementation of the selected changes. This includes planning to get approval and buy-in for changes; planning for sustainability; and creating a task-oriented timeline for implementing changes and assigning tasks. The task force convenes for a final meeting to review progress in implementation, and plan any next steps for the group, such as checking in on implementation or transitioning to a wellness team.
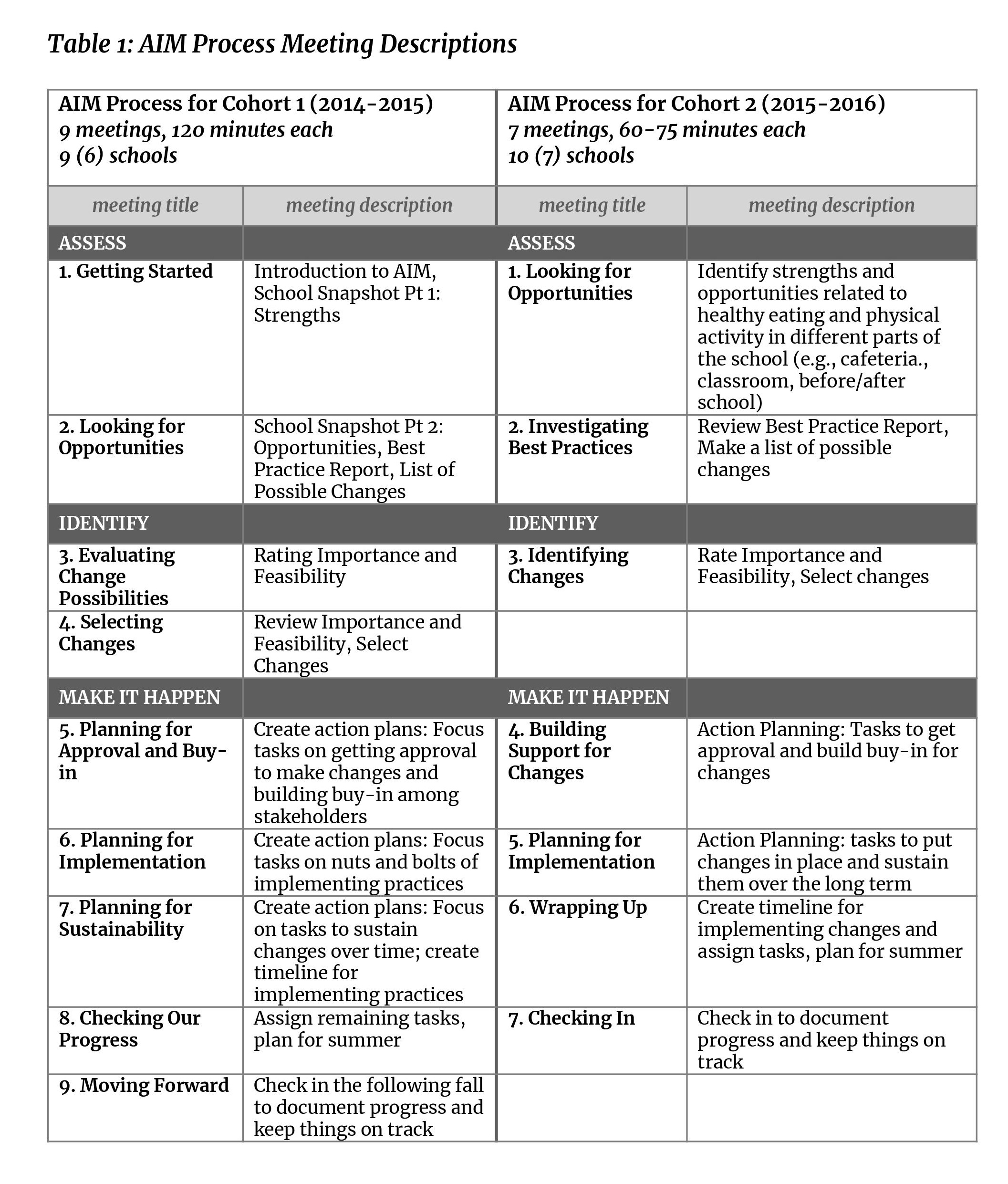
The AIM process was implemented with two separate cohorts and revised between cohorts 1 (8 schools) and 2 (10 schools) based on feedback from facilitators and task force members. The most significant revision was the amount of time dedicated to AIM meetings and activities; the number of meetings was reduced from 9 to 7 meetings, and the length of meetings was reduced from 120 to 60-75 minutes (see Table 1: AIM Process Meeting Descriptions).
Program setting.
This study took place from 2014-2016 in a rural/frontier plains region in Colorado encompassing 7 counties and 15,962 square miles (larger than the state of Maryland) that includes the lowest county health rankings and highest childhood poverty rates in the state (Robert Wood Johnson Foundation, 2020).
Program recruitment.
Project staff recruited LPHAs and schools through in-person visits at each site during the academic school year preceding the intervention. School recruitment meetings were typically attended by the school principal and physical education teacher. Schools received $4,000 to complete the AIM process. LPHA recruitment meetings were attended by agency directors and staff identified as potential AIM facilitators, who were in most cases nurses. Informational flyers explaining the AIM process and Memorandums of Understanding were key artifacts used during recruitment efforts. LPHAs were remunerated at 10% FTE of the individual(s) facilitating schools for each school facilitated through the AIM process (e.g., one school facilitated through AIM by a LPHA employee earning $50,000 resulted in a $5,000 payment to the LPHA).
LPHAs also participated in a readiness assessment interview during the recruitment phase, which provided an opportunity to discuss their motivations and reservations to participating. LPHAs noted the shared priority of addressing obesity (all 5 included obesity in their most recent Health Assessment Plans) and the potential benefits of closely collaborating with schools in their service area.
Training and technical assistance for LPHAs.
LPHA directors designated staff to facilitate the AIM process. LPHA staff were trained through a five-day training in August and a one-day booster training midway through the school year. Two facilitators who worked with both cohort 1 and cohort 2 attended a one-day training focused on revisions from the previous year in lieu of attending the five-day training a second time. Ongoing support to discuss progress and answer questions consisted of monthly conference calls among facilitators and university staff, and individualized ad hoc technical assistance (see Meyers et al., 2012).
Process and outcome evaluation design
This study used a process and outcome evaluation approach to monitor and evaluate the implementation of the AIM process (Handley et al., 2016). Process evaluation efforts, which were guided by the RE-AIM framework (Glasgow et al., 1999), began with the recruitment of LPHAs and schools and ended 6 months after all participating schools had completed the AIM process. Outcome evaluation was focused on the implementation of evidence-based practices in participating schools and general satisfaction with the AIM process and facilitators. This study was approved by the Colorado Multiple Institution Review Board.
Data collection
1. Post-meeting surveys (AIM facilitators).
All AIM facilitators (LPHA staff and university staff) completed a post-meeting survey at the end of each AIM meeting. These surveys included attention to logistical aspects of the meeting (date, time, and length of the meeting); facilitator preparation; fidelity to the meeting guide; task force dynamics (member participation and tension during the meeting); and feedback about the meeting agenda and process. There was an average of 33 items per post-meeting survey. Implementation status of changes was included in the final AIM meeting survey.
2. Post-intervention interviews (AIM facilitators).
All AIM facilitators participated in a semi-structured interview at the end of the intervention. These interviews were held in person at the health agency office or in a community setting and focused on LPHA facilitator perspectives on four topics: 1) facilitation of the AIM process at the school, 2) partnership with the university team, 3) impacts on the agency or its personnel, and 4) suggested improvements to the AIM process.
3. Post-process survey (AIM task force members).
Those participating in the AIM process and serving on the AIM task force completed a 53-item survey at the end of the AIM process. Key topics included in this survey were perceptions of the facilitator and overall satisfaction with the AIM process.
4. Process documentation.
Other data, correspondence, meeting notes, and artifacts that document the process were collected throughout the intervention to inform and contextualize dimensions of the intervention as guided by the RE-AIM framework.
Data analysis
Evidence-based practices were coded as nutrition or physical activity by the task forces proposing the changes. These practices were then coded to the sub-areas of changes by two researchers. Discrepancies in coding were identified and discussed by raters to determine the final coding.
Interviews with LPHAs were transcribed and analyzed using structural, open, and axial coding. (Glaser & Strauss, 2009; Tolley et al., 2016). Two researchers completed the analysis, with regular meetings to identify inconsistencies and discrepancies in coding and to discuss emergent themes (Houston et al., 2010). Project documents and records were analyzed by researchers to ensure the accurate and complete depiction of the intervention as it unfolded.
{kind=link}