Although numerous antibiotics have been developed and used in the treatment of bacterial infections for near a century, bacterial infections and multidrug-resistant bacteria are still pressing public health concerns[1, 2]. Increasing numbers of multidrug-resistant bacteria may be due to the overuse of antibiotics and increased potential risks from invasive surgery or therapy processes[3]. For decreasing the unnecessary usage of antibiotic therapy, a critical issue is differentiating bacterial infection from sterile inflammation accurately, because the treatments for infection and sterile inflammation are diametrically different in the clinic. However, rapid and accurate technologies for early detection and localization of infections in the patient remain a challenge. Traditional tools such as microscopy based on culturing of tissue biopsies or blood samples are not accurate enough, because of the sampling error/bias, furthermore, such methods are most suitable for the later stage of infection[4]. Therefore, noninvasive imaging methods are necessary, and structural imaging techniques such as X-ray, computed tomography (CT), magnetic resonance imaging (MRI) have been applied in infection diagnosis. These techniques are based on the presence of abnormal fluid that occurred late within tissues. However, the abnormal fluid may also appear under but sterile inflammatory conditions[5]. Therefore, these techniques are nonspecific, cannot differentiate infections from inflammation[6].
Nuclear medicine imaging, positron emission tomography (PET), and single positron emission tomography (SPECT) have also been used in infection diagnosis currently[7]. Combined with CT or MRI for anatomical reference, PET-CT, PET-MRI, or SPECT-CT can provide unprecedented sensitivity (nano-to picomolar) and quantifiable readout to deep-seated infections[8–10]. Moreover, PET/SPECT imaging is excelling at visualizing infectious pathophysiology in the early stage beyond structural imaging and evaluating the efficacy of therapeutic regimens. Consequently, many bacteria-specific radiotracers designed for infection imaging have been developed. Several reviews have summarized the metabolic pathways and molecule targets in bacteria of the available radiotracers[11–13]. In general, radiotracers designed for infection imaging are building upon the following aspects in bacteria: (1) Carbohydrate catabolism: 2-18F-fluorodeoxysorbitol (18F-FDS)[14, 15], 18F-maltohexaose (MH18F)[16], and 6″-18F-fluoromaltotriose[17]; (2) Bacteria folate biosynthesis: 11C-para-aminobenzoic acid (11C-PABA)[18], 2-18F-para-aminobenzoic acid (2-18F-PABA)[5, 19], and 18F-Fluoropropyl-trimethoprim (18F-FPTMP)[20]; (3) Iron transport systems in bacteria: 68Ga-pyoverdine PAO1(68Ga-PVD-PAO1)[21]; (4) Bacterial thymidine kinase in bacteria: 124/125I-1-(2′-Deoxy-2′-fluoro-β-D-arabinofuranosyl)-5-iodoracil (124/125I-FIAU)[22]; (5) Components of cell wall: D-methyl-11C-methionine (11C-D-Met)[22], D-3-11C-Alanine[23]; (6) Antimicrobial peptides: 99mTc-UBI-29-41[24] and 68Ga-UBI-29-41[25]. Although many bacteria-specific tracers have been developed, some of them exhibit good outcomes in infection imaging and show strong clinic potential. However, there are also limitations of these tracers, such as low specificity in patients, limited differentiating ability of particular bacterial strains and dependent on bacterial metabolic state for some tracers. Thus, it is important to exploit potential targets of bacteria for infection imaging.
In this study, bacterial nitroreductase (NTR) was selected as a new target for infection imaging. NTR is a family of flavin-containing enzymes, widely exist in most Gram-positive, Gram-negative bacteria and hypoxia tumors[26, 27]. Aromatic nitro groups can be reduced to nitroso group, hydroxylamine group, and the amino group ultimately under the catalysis of NTR[28]. In this reductive reaction, reduced nicotinamide adenine dinucleotide (NADH) or nicotinamide adenine dinucleotide phosphate (NADPH) is a vital cofactor, provide electrons in the reduction process[29]. Notably, NTR is also recognized as a biomarker of bacterial infection in clinical, food, and environmental samples. Up to now, NTR-activated imaging tools have attracted great attention for infection imaging, include electrochemical and fluorescent imaging[30–32]. Although NTR activated optical imaging probes used in infection imaging have already been well described and studied, radiotracers responsive to bacterial NTR for detecting and localizing deep-seated infections in vivo are still scarce.
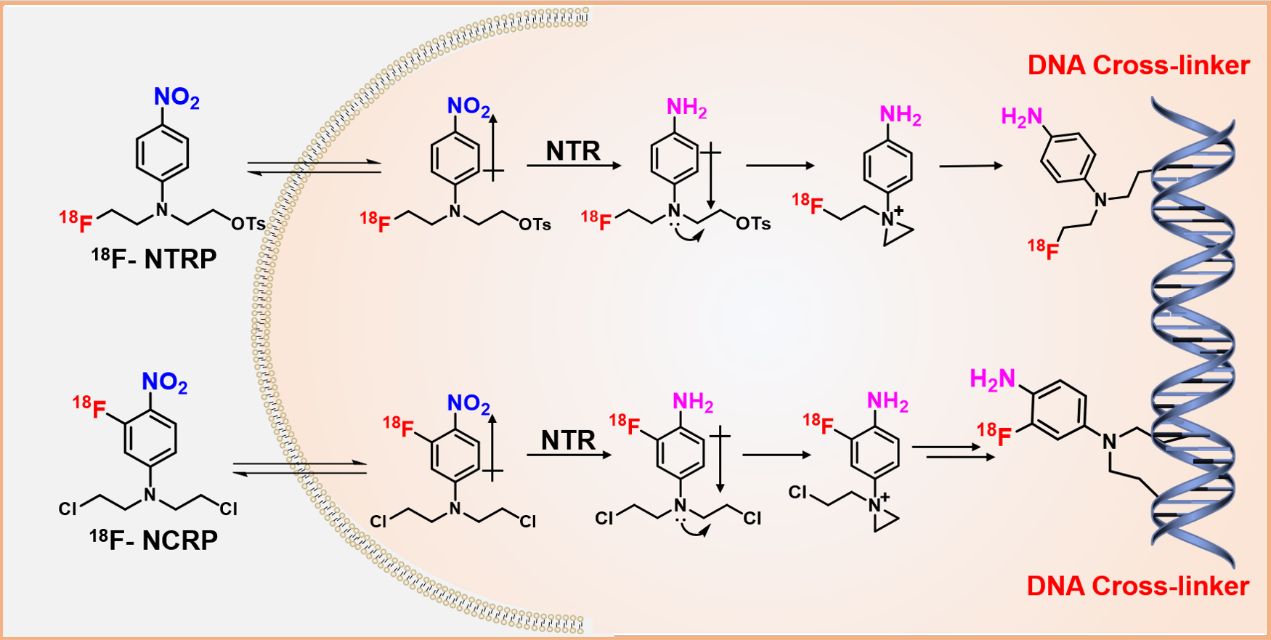
Herein, we designed and radiolabeled two NTR activated tracers, nitrogen mustard analogues decorated with aromatic nitro groups (18F-NTRP and 18F-NCRP), as new PET tracers applied for infection imaging. 18F-NTRP and 18F-NCRP are consists of two separate functional domains: an efficient NTR responsive moiety “aromatic nitro group” and a potential trapped effector “nitrogen mustard”. Nitro is a kind of strong electro-withdrawing group, decreases the electron density of nitrogen mustard required for alkylation. In bacterial infection sites, the nitro group of 18F-NTRP or 18F-NCRP is likely to be reduced to electron-donating group amino with NTR specifically. After that, the lone pair electrons developed on nitrogen mustard are conducive to the formation of a highly electrophilic aziridinium ring, which enables cross-link to bacterial DNA through covalent bond.
In this study, we developed fully automated radiosynthesis methods of 18F-NTRP and 18F-NCRP, which consistently yielded the final products in large quantity with high radiochemical purity (RCP) and molar activity. Both 18F-NTRP and 18F-NCRP were specifically reduced by NTR and readily taken up and retained by bacteria. Escherichia coli (E. coli) and Staphylococcus aureus (S. aureus) were chosen as representative Gram-negative and Gram-positive bacteria and typically overexpress NTR[33]. PET imaging in E. coli and S. aureus infected mice models were also performed with 18F-NTRP and 18F-NCRP. In addition, many frequently encountered infections are caused by E. coli and S. aureus, such as pneumonia, diarrhea, superinfection, and osteomyelitis, etc.[34, 35]. We also performed PET imaging noninvasively differentiate infection in vivo from sterile inflammation with 18F-NTRP and 18F-NCRP. Therefore, we think 18F-NTRP and 18F-NCRP having outstanding performance in early detecting, and specifically locating infections in vivo.
{kind=link}