This study of patients presenting with respiratory distress examined causal discharge diagnoses, the diagnostic accuracy of EMS physicians in an out-of-hospital setting, and hospital mortality. Our data show that diagnostic accuracy and hospital mortality differ widely depending on the discharge diagnoses. Overall, the high portions of misdiagnosis and the high hospital mortality rate confirm the assumption that this patient population seems to be particularly challenging and critically ill.
Discharge diagnoses and diagnostic accuracy of the PEMT
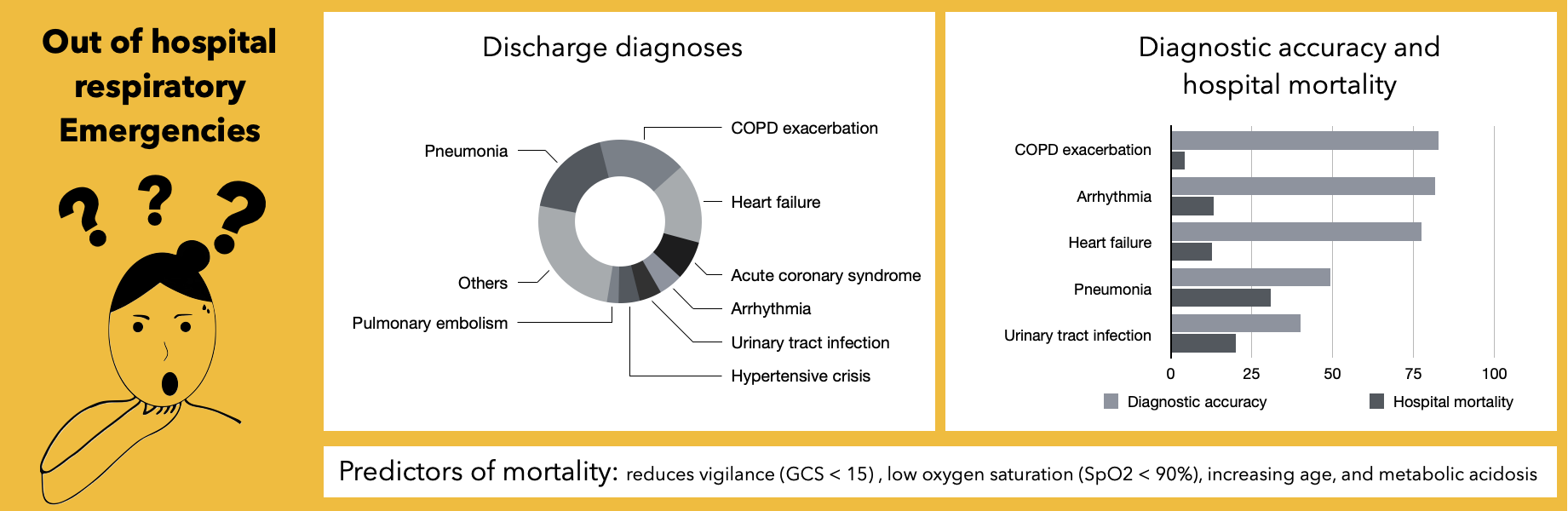
The high proportion of 24.1% of all PEMT encounters during the study period shows the great relevance of nontraumatic respiratory emergencies in the daily routine of EMS. The highest prevalence was found for pneumonia, COPD exacerbation, and decompensated heart failure. This is largely consistent with the results of comparable out-of-hospital (5, 6) and emergency department (7, 8) studies. Seven other discharge diagnoses accounted for more than 25% of PEMT encounters in our study. This demonstrates that EMS professionals must consider a wide range of differential diagnoses when treating patients with respiratory distress.
Studies assessing the diagnostic accuracy of EMS professionals in respiratory emergencies are rare and differ in the way diagnostic accuracy was calculated.
In our survey, the overall proportion of PEMT misdiagnoses was 30.1%. In two former PEMT studies from Germany, the highest portions for misdiagnosis (26% and 41%) were found in patients admitted for dyspnea (10, 11). In contrast, two other German PEMT studies observed the highest misdiagnosis rates in neurological emergencies (13, 14). Interestingly, these studies did not show a notable accumulation of misdiagnoses in respiratory emergencies. It is noticeable that one of them – the study by Arntz et al. (13) - differs in the qualifications of the EMS physicians involved. While 68% of the EMS physicians in this study were internists, only anesthesiologists worked as EMS physicians in all other studies (including ours). The strikingly low misdiagnosis rate described by Arntz et al. may be because internist-trained EMS physicians have more clinical experience in diagnosing patients with respiratory problems.
Looking at the individual discharge diagnoses in our study, there were huge differences in diagnostic confidence. Low diagnostic accuracy is particularly notable for pneumonia, which was the most frequent discharge diagnosis in our study. Pneumonia was also associated with the highest hospital mortality rate (31%), the highest rate of ICU admissions (37.3%), and a significantly increased likelihood of in-hospital death. This observation is supported by the paramedic study by Kauppi et al., which also found that patients with respiratory distress due to pneumonia had the highest mortality (5). Our analysis of PEMT misdiagnoses found that EMS physicians often suspected COPD exacerbation or decompensated heart failure when pneumonia was actually present.
It is less surprising that diagnostic accuracy was low for urinary tract infection. Presumably, few EMS professionals think primarily of a urinary tract infection in patients presenting with respiratory distress. However, patients admitted with urinary tract infection showed the second highest mortality rate of 20%. Closer examination of these cases revealed that a second discharge diagnosis (e.g., COPD exacerbation, pneumonia, and decompensated heart failure) was made in 12 of 35 patients admitted with a urinary tract infection. In these cases, it cannot be excluded that the respiratory symptoms were caused by these second discharge diagnoses. Urinary tract infections were at least concomitantly present in 4.9% of analyzed PEMT encounters and should therefore be considered a relevant differential diagnosis and cause for respiratory distress.
One former emergency department study of elderly patients with respiratory distress described that misdiagnosis resulted in worse patient outcomes (9). In our study, the EMS physician made an incorrect diagnosis in 42.7% of all cases of in-hospital death. Using logistic regression, we found that an incorrect out-of-hospital diagnosis was associated with a significantly increased probability of hospital mortality. It can therefore be suspected that an increase in diagnostic accuracy would result in a decrease in morbidity and mortality.
Pathological findings associated with discharge diagnoses
The two strongest associations we found were of prehospital wheezing being strongly associated with asthma (odds ratio 38.8) and lower extremity edema being associated with decompensated heart failure (odds ratio 13.7). Our data indicate that a clear recommendation can be made for thorough auscultation of the lungs and evaluation of lower extremity edema in all patients with respiratory distress.
Several findings correlated with low or moderate odds ratios with discharge diagnoses. It became clear that many routine parameters (e.g., body temperature and GCS) provide important information about discharge diagnoses. Nevertheless, some of these parameters were not documented in many encounters. Our results indicate that measurement of all these routine parameters in any respiratory emergency is advisable. This even allows for the identification of unexpected pathological findings (e.g., high body temperature), which can provide essential hints for the correct diagnosis.
Because out-of-hospital diagnosis can be very challenging, a diagnostic algorithm seems to be useful to identify the correct diagnosis and initiate appropriate therapy. Further studies on the relationships between examination findings, medical history, and discharge diagnoses could aid development of an effective diagnostic algorithm. In addition, EMS professionals should be better prepared for the challenging diagnosis of respiratory emergencies through focused education and training in the future.
Some emergency department studies have shown that the use of point-of-care ultrasound (POCUS) in respiratory emergencies can reduce the number of differential diagnoses and increase diagnostic accuracy (15–17). Out-of-hospital use of ultrasound and training of EMS professionals in POCUS therefore have the potential to increase diagnostic confidence.
Hospital mortality and the search for associated predictors
The hospital mortality rate in our study was 13.8%, which was comparable to that of three similar EMS studies from Scandinavia involving patients with dyspnea (1, 4, 5). These studies reported hospital or 30-day mortality rates of 11%, 12.3% and 13.2%, respectively. We attribute the slightly higher mortality in our study to the fact that only EMS encounters involving EMS physicians were analyzed and that these encounters presumably represent a particularly critical subset of all respiratory emergencies. Unsurprisingly, the ICU admission rate in our study was also very high (22.4%). The consistent above-average mortality and ICU admission rates highlight that patients with respiratory distress should be considered high-risk.
According to our analysis, decreased vigilance, low oxygen saturation, and increasing age can be considered independent predictors for hospital mortality. Two former emergency department studies that included patients with any complaint also found that decreased vigilance was an independent risk factor for 30-day mortality (3, 18). The same conclusion was made in an EMS study of patients with the complaint of dyspnea (19). Two of these studies (3, 19) similarly reported that low oxygen saturation was a risk factor for mortality. Patients with dyspnea have a higher risk of death with increasing age, which has also been shown by previous studies (9, 19).
Hospital mortality and initial blood gas analysis
Examination of the initial BGA results shows that metabolic acidosis appears to be a strong risk factor for death. Closer examination demonstrated that both lactate acidosis and metabolic acidosis of another origin showed this association.
Surprisingly, there is little evidence of the prognostic value of BGA results in patients with respiratory distress. Two previous studies showed that acidosis led to a higher risk of mortality or ICU admission in patients with dyspnea (20, 21). That initial hyperlactatemia is an independent predictor of mortality in unselected emergency department patients has been demonstrated by numerous studies (22–24). Our results highlight that elevated lactate is an important prognostic parameter even in emergency patients with respiratory distress. Therefore, BGA, including lactate, should be routinely measured in all patients presenting with respiratory distress.
Limitations
Compared to other studies, our study is based on a relatively small sample size. Because we examined only PEMT encounters during winter and spring, our results do not allow for conclusions about all respiratory emergencies throughout an entire year. Rather, it can be assumed that we studied a particularly critically ill subset of this patient population. Since the evaluation of diagnostic accuracy was not blinded, it cannot be excluded with certainty that it was over- or underestimated. The many missing data in some examination findings posed challenges for the multivariable analyses. We tried to compensate them by running multiple imputations. The sample size for BGA analysis was particularly small, as BGA results were obtained from only half and lactate was measured in a quarter of the encounters.
{kind=link}