Outcomes and baseline characteristics of serum biomarkers of RM in patients who underwent EHS stratified according to the incidence of AKI
A total of 187 patients were included, and all of them were males. Of these, 82 (43.9%) patients had AKI at admission, and stage 1, stage 2 and stage 3 were 62/82 (75.6%), 11/82 (13.4%) and 9/82 (11.0%), respectively. Twenty-one (12.4%) patients had AKI at discharge, and 10/21 (47.6%), 6/21 (28.6%) and 5/21 (23.8%) patients had stage 1, stage 2 and stage 3 AKI, respectively. The 90-day mortality was higher in AKI than in non-AKI (26.8% vs. 1.0%, P<0.001). The levels of MB and CK at admission, 24 hours, 48 hours, and discharge were higher in patients with AKI than in non-AKI patients. (Table 1).
Table 1
Clinical serum biomarker of rhabdomyolysis and outcomes of patients who underwent EHS, stratified according to incidence of acute kidney injury
| Variables | Non-AKI(n=105) | AKI(n=82) | P value |
| Age (years), Mean (SD) | 23.6 ± 8.0 | 26.1 ± 11.0 | 0.128 |
| Males, N (%) | 105(100%) | 82(100%) | 1.000 |
| Outcomes N (%) | | | |
| AKI at admission | | 82/187 (43.9%) | |
| Stage 1 | | 62/82 (75.6%) | |
| Stage 2 | | 11/82 (13.4%) | |
| Stage 3 | | 9/82 (11.0%) | |
| AKI discharge | | 21/169 (12.4%) | |
| Stage 1 | | 10/21(47.6%) | |
| Stage 2 | | 6/21(28.6%) | |
| Stage 3 | | 5/21(23.8%) | |
| 90-day mortality | 1/105 (1.0%) | 22/82 (26.8%) | <0.001 |
| Serum biomarker of RM | | | |
| MB (ng/ml), median (IQR) | | | |
| admission | 193.6 (63.2–583.5) | 1000.0 (469.9–1000.0) | <0.001 |
| 24 hours | 68.8 (24.0–206.6) | 461.8 (142.0–1000.0) | <0.001 |
| 48 hours | 61.0 (33.5–298.1) | 485.0 (188.8–1000.0) | <0.001 |
| Discharge | 38.5 (21.0–76.5) | 516.0 (90.0–1000.0) | <0.001 |
| CK(U/L), median (IQR) | | | |
| admission | 793.5 (248.5–2148.2) | 1119.0 (483.0–3518.0) | 0.028 |
| 24 hours | 716.5 (233.5–2531.8) | 2083.0 (822.0–4768.5) | <0.001 |
| 48 hours | 61.0 (33.5–298.1) | 485.0 (188.8–1000.0) | 0.005 |
| Discharge | 38.5 (21.0–76.5) | 516.0 (90.0–1000.0) | 0.036 |
| CK-Mb (ng/ml), median (IQR) | | | |
| admission | 32.5 (22.0–59.8) | 45.0 (29.0–101.5) | 0.007 |
| 24 hours | 32.5 (17.2–62.0) | 57.0 (32.0–104.5) | 0.003 |
| 48 hours | 28.0 (21.0–60.0) | 40.0 (21.0–73.0) | 0.284 |
| Discharge | 13.0 (8.8–19.0) | 16.0 (7.7–30.5) | 0.214 |
Association of Myoglobin and Acute Kidney Injury and 90-day Mortality Following Exertional Heatstroke
The characteristics of the patients, stratified according to quartiles of myoglobin level, are shown in Figure 1. For rhabdomyolysis after heatstroke, the incidence of AKI was 73.08% in the highest myoglobin quartile (≥1000 ng/ml) and 12.82% in the lowest quartile (<127 ng/ml), which yielded an adjusted odds ratio of AKI that was 18.95 (95% confidence interval [CI], 6.00–59.83) times as high in the highest quartile as in the lowest quartile (Fig. 1). The myoglobin level was also strongly associated with the combined outcome of acute kidney injury and death at 90 days (adjusted odds ratio, 7.9; 95% CI, 1.61 to 38.89) (Fig. 2).
Myoglobin is Associated with HK-2 Cell Ferroptosis in a Heat Stress Model
To determine the role of myoglobin in the mechanism of human kidney proximal tubular (HK-2) cell function, HK-2 cells were treated with myoglobin at concentrations of 882.35nm/l at 43 ℃ for 2 hours and rewarmed at 37 ℃ at different time points (0 h, 1 h, 3 h, 6 h, and 12 h). First, we examined the effect of heat shock and myoglobin on the survival of HK-2 cells, and the cell survival rate began to decline after 0 h of rewarming (Fig. 3A, P < 0.01). Simultaneously, with the extension of rewarming time, the cell survival rate decreased significantly; after 12 h of rewarming, the cell survival rate decreased to less than 50%. We further determined whether ferroptosis was involved in severe heatstroke complicated with AKI. P53, SLC7A11 and GPX4 expression in HK-2 cells was detected by Western blot. We found that compared with the control group at 37 ℃, the expression of p53 was significantly increased in response to myoglobin after heat stress for 0 h. With the extension of rewarming time, the expression increased and then decreased and reached its highest level at 3 h of rewarming (Fig. 3B, P < 0.01). As shown in Figure 1C, the expression of SLC7A11 and GPX4 was significantly decreased after heat stress and myoglobin treatment for 0 h, and the expression continuously decreased with the extension of rewarming time. Furthermore, the change in intracellular iron content is a very important indicator of ferroptosis. We evaluated HK-2 cell ferroptosis by detecting the intracellular iron content and found that intracellular Fe2+ was markedly increased at 3 h of rewarming after heat stress and myoglobin treatment (Fig. 3C, P < 0.01). Additionally, the level of ROS was significantly increased at 3 h of rewarming in the heat stress- and myoglobin-treated cell model, suggesting that heat shock and myoglobin could induce the production of ROS and activate oxidative stress in HK-2 cells (Fig. 3D, P < 0.01). Then, silencing of the P53 gene was used via an siRNA approach. SLC7A11 and GPX4 expression in HK-2 cells was significantly decreased at 3 h of rewarming in response to myoglobin under heat stress, and these effects were prevented by P53 gene silencing in HK-2 cells (Fig. 3E, P < 0.01). Taken together, our data show that myoglobin appears to be related to human HK-2 cell ferroptosis under heat stress by affecting SLC7A11 and GPX4 expression, intracellular iron content, and the production of ROS.
Myoglobin aggravates the Endoplasmic Reticulum Stress (ERS) Response of HK-2 cells after Heat Stress
We further analysed the expression of ERS-related proteins by Western blot, mainly detected the three classical pathways of ERS, and analysed the expression of ATF-4, CHOP, ATF-6, IRE1 and p-IRE1. HK-2 cells treated with myoglobin and heat stress showed elevated expression of p-IRE1/IRE1, ATF-4, ATF-6 and CHOP, and with the extension of rewarming time, their expression first increased and then decreased (Fig. 4A, P < 0.01). To confirm this, we used an ERS inhibitor (4-BPA) to treat HK-2 cells. There was a significant increase in the expression of p-PER/PERK, p-eIF2, p-IRE1/IRE1, ATF-4, ATF-6 and CHOP at 3 h of rewarming in response to myoglobin under heat stress; thus, pretreatment with 4-BPA markedly decreased the expression of p-PER/PERK, p-eIF2, p-IRE1/IRE1, ATF-4, ATF-6 and CHOP in the heat stress and myoglobin groups (Fig. 4B, P < 0.01). Together, these data reveal the important role of myoglobin in aggravating the ERS response in HK-2 cells during heatstroke.
Myoglobin modulates HK-2 cell Ferroptosis involving Endoplasmic Reticulum Stress after Heat Stress
ERS is closely related to ferroptosis. The above results suggest that both ERS and ferroptosis are involved in the process of heat stress- and myoglobin-mediated renal tubular injury, but the definite regulatory mechanism is not clear. To address whether myoglobin modulates ferroptosis by interacting with ERS, we performed 4-BPA to pull down ERS activation in HK-2 cells before heat stress and myoglobin treatment. We found that the cell survival rate was significantly decreased after heat stress and myoglobin treatment rewarming for 3 h, and the cell survival rate was markedly increased in the 4-BPA + myoglobin+ heat stress group (Fig. 5A, P < 0.01). Western blot analysis showed that inhibition of ERS using 4-BPA decreased p53 activation and enhanced SLC7A11 and GPX4 expression in HK-2 cells after heat stress and myoglobin treatment (Fig. 5B, P < 0.01). Notably, intracellular Fe2+ and ROS were significantly decreased in response to heat stress and myoglobin combined with 4-BPA treatment rewarming for 3 hours (Fig. 5C and D, P < 0.01), indicating that inhibiting ERS could suppress the accumulation of iron and ROS production induced by myoglobin under heat stress.
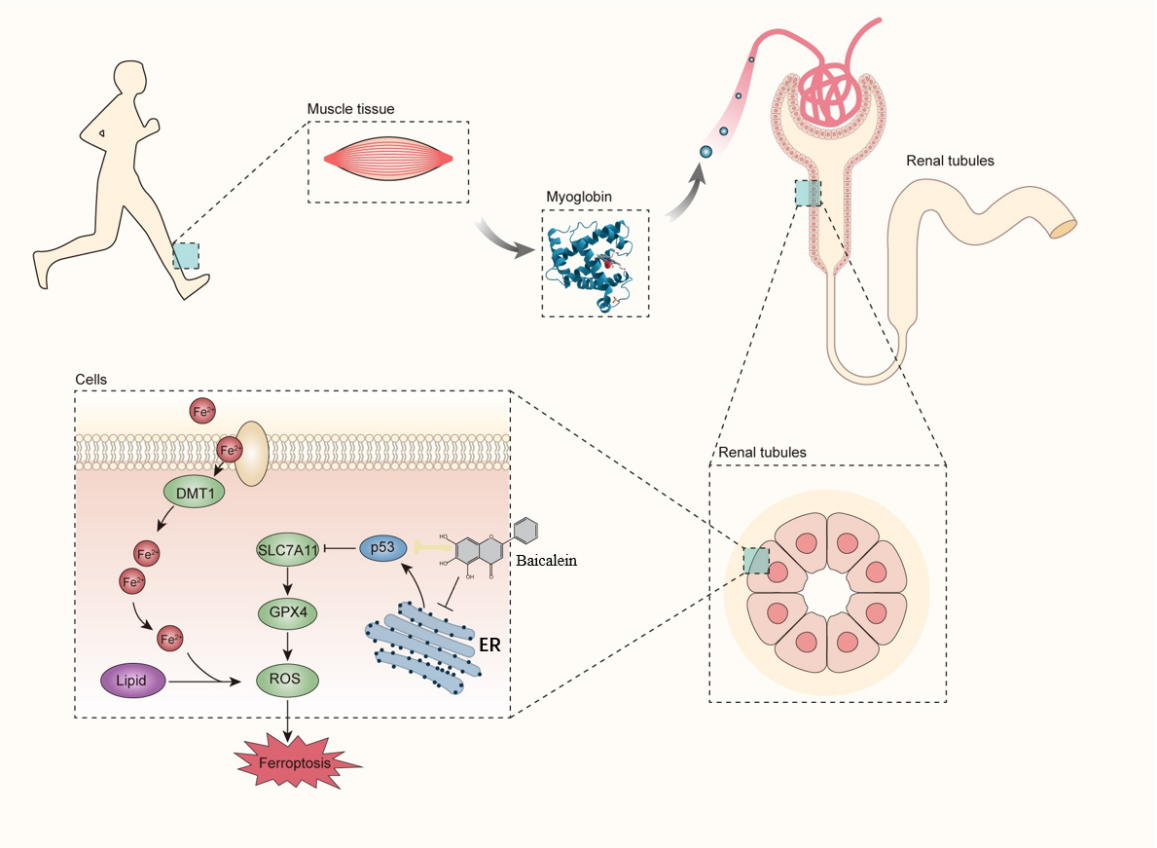
Baicalein Protects HK-2 Cell Ferroptosis Induced by Myoglobin under Heat Stress by Inhibiting Endoplasmic Reticulum Stress
Recent studies have reported that ERS and ferroptosis are involved in AKI induced by heat stress combined with myoglobin, and ERS inhibitors can effectively inhibit ferroptosis and alleviate heat stress and myoglobin-mediated kidney injury. Therefore, we considered whether there are clinical drugs that can inhibit ferroptosis by regulating ERS to alleviate rhabdomyolysis-induced AKI after EHS. Previous studies have shown that baicalein can inhibit ferroptosis during tumours, sepsis and hypoxic renal injury [31–33], but its mechanism is not completely clear. In the present study, as expected, treatment with baicalein increased the cell survival rate after heat stress and myoglobin treatment rewarming for 3 h (Fig. 6A, P < 0.01), suggesting the protective role of baicalein in AKI under heat stress. Furthermore, baicalein inhibited the activation of ERS signalling, as demonstrated by decreased expression of p-PER/PERK, p-eIF2, p-IRE1/IRE1, ATF-4, ATF-6 and CHOP in the heat stress and myoglobin treatment rewarming for 3 h group (Fig. 6B, P < 0.01). Simultaneously, baicalein alleviated ferroptosis in HK-2 cells, as shown by decreased p53 activation and elevated SLC7A11 and GPX4 expression (Fig. 6C, P < 0.01). Notably, intracellular Fe2+ and ROS were markedly decreased in response to heat stress and myoglobin combined with baicalein treatment rewarming for 3 hours (Fig. 6D and E, P < 0.01), indicating that baicalein could inhibit the accumulation of iron and ROS production induced by myoglobin under heat stress.
{kind=link}