Primary hepatic NEC is a very rare tumor, even among gastro-enteropancreatic neuroendocrine neoplasms (GEP-NEN); its incidence is reportedly 0.3% among all NEN, and 0.46% among primary hepatic malignancies [7]. As the liver is the most frequent site of NEN metastases from other organs, a systemic search for the primary lesion is necessary when hepatic NEN was suspected, considering the rarity of PHNEC. In contrast, HCC, the most common liver malignancy, often coexists with other malignancies. The most common of these combinations, at 2.0–3.6% of all primary hepatic malignancies, is HCC with intrahepatic cholangiocarcinoma [8].
Although the exact origin of PHNEC is unclear, two hypotheses have been proposed [9, 10]: (a) neuroendocrine cells in the intrahepatic bile-duct epithelium undergo malignant conversion and become PHNEC; and (b) PHNEC originates from stem cells that dedifferentiated from other malignant hepatic cells and convert into neuroendocrine cells. The latter concept can explain the lesions with different carcinomas in one site, whereas the former can only explain the pathogenesis of single PHNEC tumors.
In the literature, these composite liver tumors are classified as either collision type or combined type. In collision-type tumors, the HCC and NEC grow as separable, microscopically distinctly compartments. In combined-type tumors, the HCC and NEC are closely intermingled, and a transition zone can be found. These tumors used to be categorized as “mixed adeno-neuroendocrine carcinoma (MANEC)” when at least 30% of either component is identified [10]. However, with the revision of the WHO Classification in 2019, “collision type” tumors, in which two components appear to be derived independently, simply adjoining with no observable mutual transition, were excluded from “mixed neuroendocrine neoplasm (MiNEN)” [11].
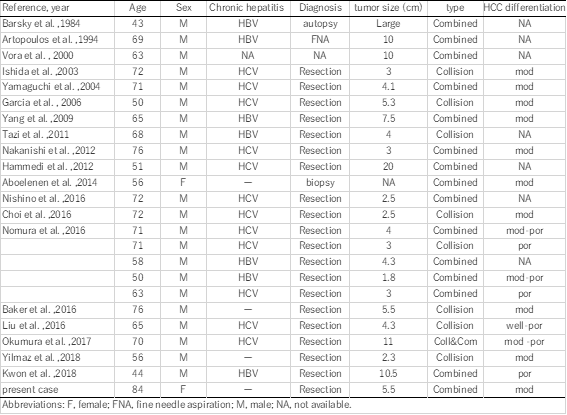
Concurrent occurrence of HCC and NEC is extremely rare. Including our patient, 21 published English-language reports of 25 patients with HCC with NEC components can be currently found. Clinicopathological profiles of these 25 patients are summarized in Table 1. These composite tumors were described as either collision type or combined type. In the present case, the two components were partly intermingled, and some portion of the HCC expressed neuroendocrine markers. Therefore, our case was classified as a combined-type MiNEN.
In the literature, combined type (n = 17) tumors were more common than collision type (n = 9; one patient had both collision- and combined-type tumors). Almost all the reported cases were preoperatively diagnosed as HCC, and re-diagnosed as combined or collision PHNEC–HCC tumors after resection, with only three cases diagnosed without surgery (by biopsy, fine needle aspiration, or autopsy); this shows the difficulty of correct preoperative diagnosis for these tumors.
In retrospective, preoperative images in the present case showed some conformity between images and pathology. In the preoperative MRI, the fatty tumor region, in which a low T1-weighted chemical shift in the dorsal tumor area is emphasized (which indicates fatty tissue and is thus highly suspicious of HCC), and the ventral area shows extremely high signal intensity in the diffusion-weighted image (typical for NEC expression) just coincide macroscopically with the distribution of HCC and NEC components in the tumor cut-surface, reflecting their mixture. Furthermore, distributions of these components show as if the HCC tumor had necrotic changes at its center, spreading to the tumor periphery. Previously, Yang et al reported a combined-type tumor in which poorly differentiated HCC focally expressed neuroendocrine marker [18], and resembled the present case. In our case, these findings seem to support the supposition that a moderate or poorly differentiated HCC transdifferentiates into a neuroendocrine phenotype, resulting in a combined HCC–NEC tumor.
The clinical significance of HCCs with NEC components is unclear. Several studies have shown that HCCs with NEC components are associated with aggressive behavior and dismal outcomes.
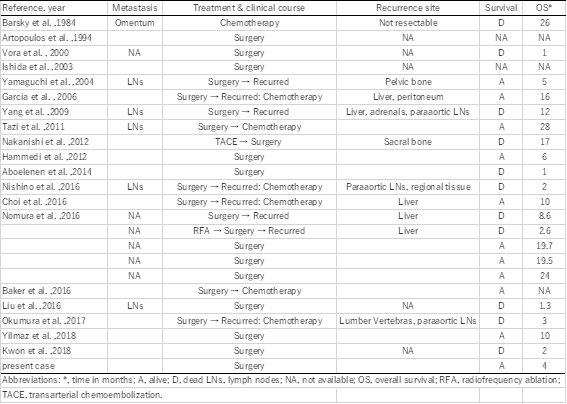
Mixed PHNEC and HCC lesions tend to have a poor prognosis. Of the 25 cases summarized, eight patients had recurrences, six patients died within a year after their surgeries, and only two patients were alive 2 years after surgery (Table 1). Although the number of reported cases is rather small, the 1-year cumulative survival rate of the patients was 53.0% in our literature review (prognosis not available for 3 patients). Among resected cases with recurrences or biopsy-confirmed metastasis, the NEC component was found in each case, which indicates that the NEC component behaves more aggressively than primary HCC, leading to a much worser prognosis. Therefore, identifying the neuroendocrine component, and assuring the patient receives proper treatment is important.
In conclusion, mixed PHNEC and HCC tumors are extremely rare. Further accumulation of case reports is required to clarify the features, diagnostic details and optimal therapy for combined PHNEC–HCC lesions.