Active inflammation promotes the development of fibrosis in CHB. Liver biopsy of chronic hepatitis showing variable necrotizing inflammation and/or fibrosis plays an important role in staging and grading CHB.20 Despite its superiority of assessing both fibrosis and inflammation in CHB,8 liver biopsy is far from an ideal gold standard because of its invasiveness, risk of complications, patient discomfort and possible unavailability due to expertise requirements.21 Staging CHB based on its severity using noninvasive tests such as elastography is important for guiding surveillance and assisting with treatment decisions.8 Noninvasive tests are being increasingly incorporated into both national and international guidelines. With its good diagnostic accuracy for significant liver fibrosis and its excellent diagnostic accuracy for liver cirrhosis,22,23 FibroScan has been widely applied. In addition to reflecting liver fibrosis, the LSM value by FibroScan (with liver biopsy as the reference standard) should also reflect changes in liver inflammation to some extent. Although it has been proven that necrotizing inflammation can lead to an increase in LSM in CHB,24,12 more strong, persuasive clinical research evidence must be collected.
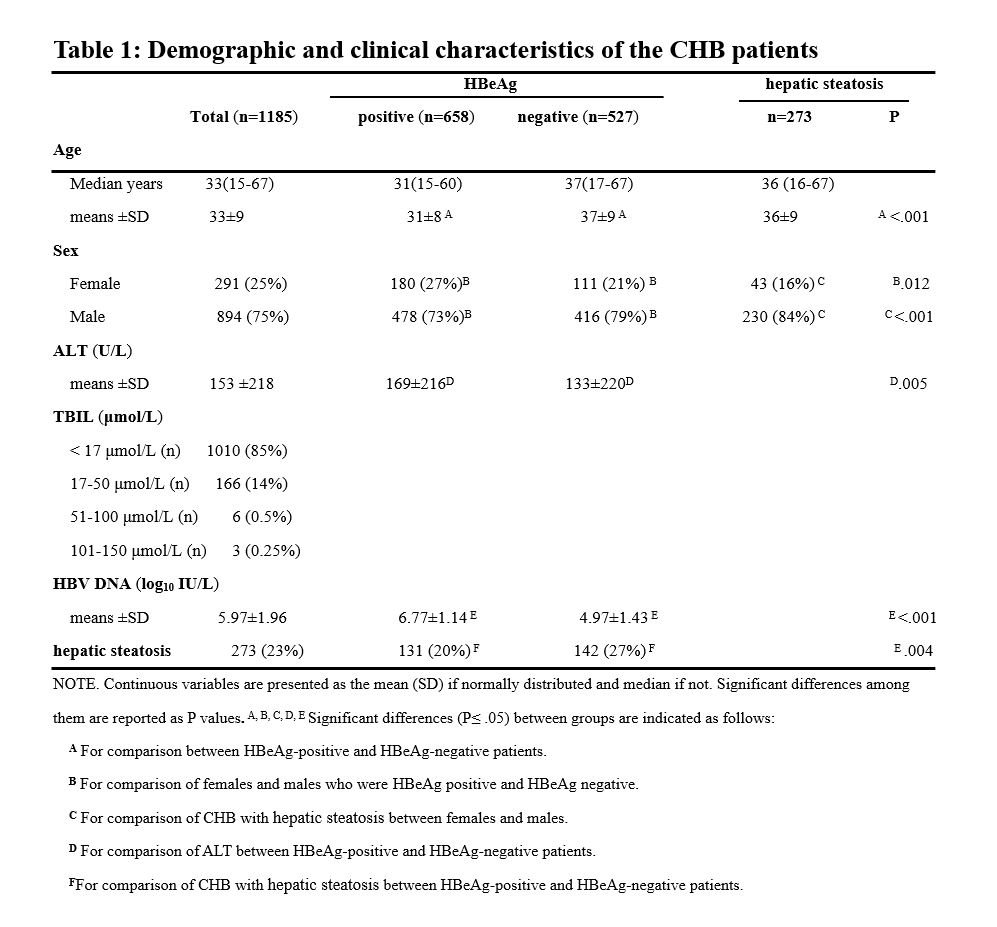
In our study, the main demographic and clinical characteristics of the 1,185 patients with CHB were consistent with previous research reports, showing good representativeness:25,1,7 the male patients accounted for 75%, the median age of HBeAg-negative CHB patients was older than that of HBeAg- positive CHB patients (P<0.001), the incidence of CHB complicated with hepatic steatosis r in men was higher (84%) than that in women (16%) (P<0.001), the incidence of the degree of hepatic steatosis in HBeAg negative group was higher than that in HBeAg positive group (P=0.004), the means±SD of ALT levels were higher in the HBeAg-positive patients than in the HBeAg-negative patients (P=0.005), the patients with a normal level range of bilirubin accounted for 85% of the total while few patients had high bilirubin levels that affect liver stiffness, and the level of HBV DNA in the HBeAg-positive patients was higher than that in the HBeAg-negative patients (P<0.001). More importantly, liver biopsy showed no difference in inflammation (P=0.082) or fibrosis (P=0.177) in patients with CHB, regardless of whether they were complicated by hepatic steatosis, which further supported the view that the presence of steatosis in CHB patients does not lead to differences in the histopathological findings.26
Usually, the performance of noninvasive diagnostic methods for liver diseases is evaluated by calculating the AUC using liver biopsy as the reference standard.11
Accordingly, the quality of liver biopsy specimens is very important. It is recommended that if applicable, the presence of fewer than 11 PAs be noted in the pathology report, with recognition that the diagnosis, grading, and staging may be incorrect due to an insufficient sample size.8,27 In our 1185 liver biopsy specimens of chronic hepatitis B, 82% had more than 10 Pas, and only 18% had fewer than 10 PAs, providing strong evidence for comparison with the noninvasive diagnosis of liver inflammation or fibrosis by FibroScan. A reliable TE assessment was defined as an assessment fulfilling three characteristics: a minimum of 10 readings, a success rate of measurements (“shots”) ≥ 60% and an IQR/median ratio (IQR/M) of ≤ 0.30.28,29,16,22 The reliability of liver stiffness evaluations depend on the IQR/M according to the median liver stiffness level17, so it is necessary to achieve a "very reliable" IQR/M (≤0.10) or the "reliable" IQR/M (0.10ཞ0.30) in the FibroScan test to the greatest extent possible. With a test success rate of over 90%, the LSM reliability results of IQR/M in the 1185 patients with CHB were 70% (IQR/M≤0.10), 23% (0.10<IQR/M≤ 0.15), 4% (0.15<IQR/M≤0.20) and 3% (0.20<IQR/M≤0.3), respectively. The more severe the liver fibrosis is, the more severe the liver inflammation is (Spearman's Rho = 0.829, P<0.001). Especially the liver inflammation of patients with cirrhosis (S4) is mostly G4, G1 and G2 are rare.
Overall, the sensitivity, specificity, misdiagnosis rate, cutoff point and AUC of LSM were compared individually, and significant differences in the LSMs were noted among different grades of liver inflammation in the 1185 CHB patients (P< 0.0001). The cutoff points and AUCs of LSMs for the diagnosis of G2, G3, and G4 were 9.6 kPa and 0.743, 9.7 kPa and 0.807, respectively, and 11.4 kPa and 0.838, respectively; that is, FibroScan could diagnose G2, G3, and G4 liver inflammation in CHB patients with LSM values of 9.6 kPa, 9.7 kPa and 11.4 kPa, respectively.
Considering that the number of PAs in liver biopsy tissues will affect the pathological diagnosis of inflammation or fibrosis of liver tissues, we also analyzed the diagnostic efficacy of FibroScan (LSM) for liver inflammation or fibrosis when PA≥10 in the liver tissues of these patients. There were significant differences in the LSMs among different grades of liver inflammation (P<0.0001). The cutoff points and the AUCs of the LSMs for the diagnosis of G2, G3, and G4 were 8.6 kPa and 0.775, 9.8 kPa and 0.818, and 11 kPa and 0.832, respectively. Significant differences were observed in the LSMs across the different stages of liver fibrosis (P<0.0001). The cutoff points and the AUCs of the LSMs for the diagnosis of S2, S3, and S4 were 8.6 kPa and 0.789, 10.4 kPa and 0.826, and 11 kPa and 0.807, respectively; that is, FibroScan could diagnose G2, G3, and G4 liver inflammation in CHB patients with LSM values of 8.6 kPa, 9.8 kPa and 11.0 kPa, respectively. In addition, the efficacy of FibroScan for the noninvasive diagnosis of liver fibrosis, especially S4, was basically consistent with international reports or guideline recommendations.30,22 Most interestingly, the LSM cutoff point for G4 liver inflammation was 11.0 kPa, which was equal to that (11.0 kPa) for the diagnosis of S4 liver fibrosis. Therefore, we believe that FibroScan has certain potential for the noninvasive diagnosis of CHB, regardless of whether liver fibrosis or liver inflammation is being evaluated.
Treatment decisions for CHB sometimes depend on the presence of necroinflammation rather than fibrosis, so the challenge is now to decide on how best to apply validated noninvasive tests in CHB management.31 ALT is used as a control liver test and serves as a nonspecific biomarker of liver injury, and serial testing of ALT levels is needed to guide treatment decisions for CHB patients.10 Due to the discomfort of blood sample collection, the poor correlation with the degree of liver disease in CHB patients, and the fact that this measurement that may fail to identify patients with necroinflammatory activity or fibrosis,32,33 serum ALT is still not the ideal biomarker for assessing the degree of liver injury in CHB patients. Comparatively, owing to its noninvasive, rapid and dynamic nature, we should not overlook the superiority of FibroScan for the evaluation of liver inflammation in CHB patients. In some reports or guidelines on the noninvasive diagnosis of liver fibrosis by FibroScan, it has been suggested that the LSM cutoff value should be adapted to the ALT level since ALT levels tend to influence the LSM in CHB34 and because ALT increases the LSM value in FibroScan and is an important factor or confounding factor affecting the accuracy of LSM, thus reducing its diagnostic efficiency.22,35 Since elevated ALT levels can reflect liver injury to some extent and necrotizing inflammation can lead to an increase in LSMs in CHB patients,24 why do we not deduce that the LSM value of FibroScan may reflect the degree of liver inflammation in addition to liver fibrosis? On the other hand, studies have shown that sustained HBV suppression with antiviral treatment can lead to a reduction in necroinflammatory activity and improvement in fibrosis stage, and CHB patients can have a significant reduction in liver stiffness during nuleos(t)ide analog treatment, even when there is little or no improvement in fibrosis according to the histologic findings.36,37 Therefore, the impact of ALT normalization by antiviral therapy has to be considered in the interpretation of the noninvasive liver fibrosis assessment results,11 which indicates that the LSM value of FibroScan reflects the recovery of liver inflammation rather than liver fibrosis in CHB patients after antiviral therapy at a certain period of time. Remarkably, different ALT levels did not affect the accuracy of the LSM for the diagnosis of liver inflammation in our study (P>0.05), so the influence of ALT on LSM should not be considered too heavily, and more attention should be given to the effect of liver inflammation on LSM. Regardless of whether liver inflammation or fibrosis is present, a decrease in the LSMs of CHB patients are welcome.
In summary, a reliance on abnormal liver function tests unfortunately causes most patients with significant liver injury to be missed,4 so noninvasive diagnostic techniques are needed to aid in CHB diagnosis and treatment monitoring. As the earliest and most extensively evaluated elastographic method for liver stiffness, FibroScan has certain potential for the noninvasive diagnosis of liver inflammation in CHB. The liver inflammation of CHB is accompanied by the occurrence and development of liver fibrosis, which was also proved in this study. It is difficult for LSM to exclude liver inflammation as an important participant in noninvasive diagnosis of liver fibrosis. In that case, we could expand the new use of LSMs for noninvasive diagnosis of liver inflammation, which was the goal of this study. This study showed that FibroScan might be a noninvasive diagnostic method for liver inflammation in CHB patients, which was better not only to expand the application field of the noninvasive diagnostic techniques of Fibroscan, but also to analyze the clinical connotation of LSM from different levels. For example, a rapid decrease of LSM in a short time after antiviral therapy is not likely to represent the remission or reversal of liver fibrosis, but more likely to be the improvement of liver inflammation in our view.
{kind=link}