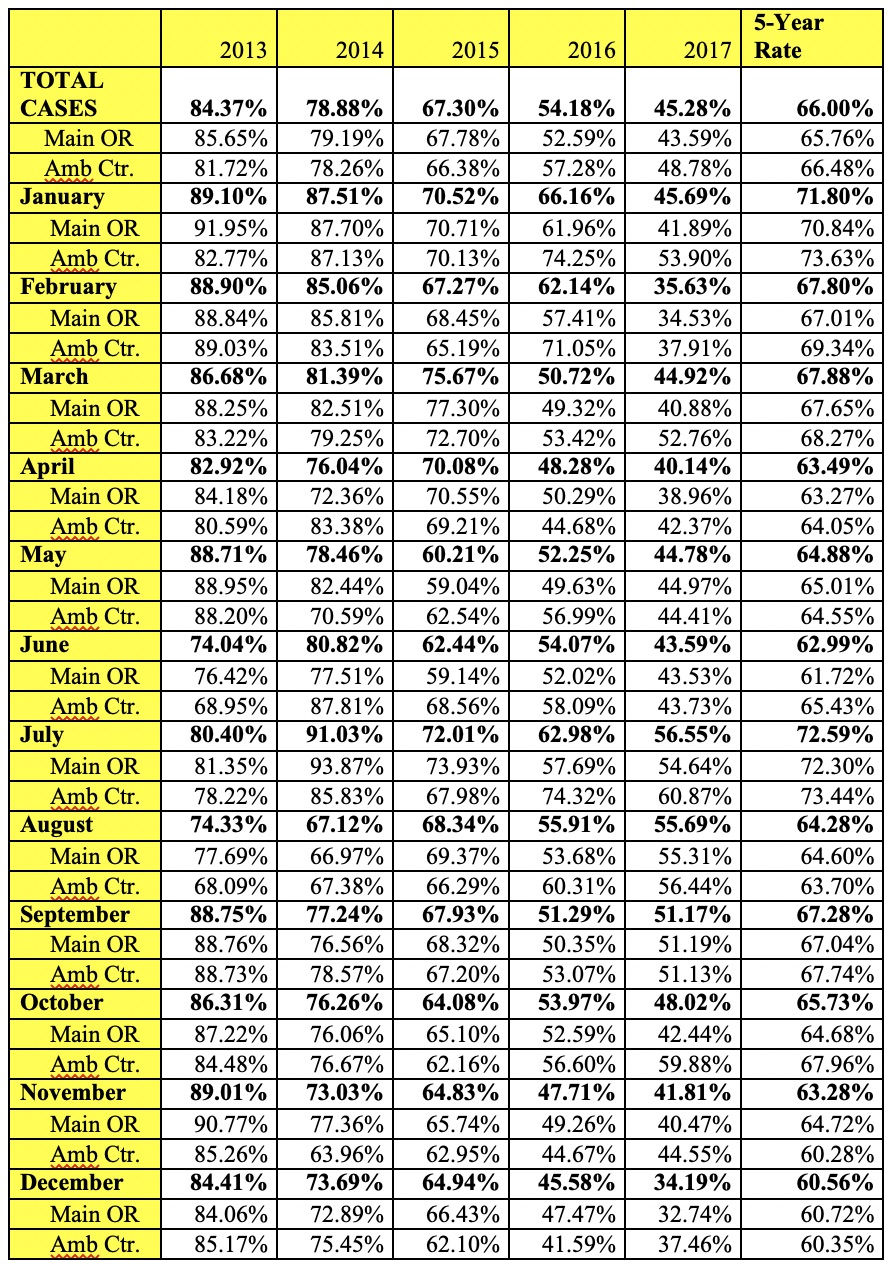
Our study aimed to analyze QA database entry rates at an institution that uses a voluntary electronic reporting structure. We found that the average rate of entry into the QA database over a five-year period was 65.51% (Table 1), a compliance level that is comparable to rates reported in the literature [3–6]. Although the primary ambulatory surgical center (Amb Ctr.) had different QA completion rates, because of the variation, a clear conclusion cannot be drawn upon whether location of anesthetic procedures affects compliance with database entry. The main Operating Room initially had a higher rate of compliance from 2013 to 2105 and later, the same day surgery center at our institution saw higher rates of QA entry after completion of the cases from 2016 to 2017 with no clear explanation.
A seasonal trend was apparent on a month-to-month basis during the 5 year period. The month of July had the highest rate of entry into the QA database with a 5 year average of 72.54%. Moreover, the greatest level of reporting for any month in the 5 year period was in July of 2014, with a rate of entry of 91%, at the beginning of the study period. This higher rate of reporting in July coincides with the start of the academic calendar for new anesthesiology residents, which may explain the increased rate of compliance. Residents may also be inclined to record cases more frequently in the QA database in July due to increased education on departmental policies regarding the QA database during this time period, especially during new resident orientation. Fear of medicolegal consequences is generally highest at the beginning of the academic year and has also been said to be a factor that influences QA reporting [6, 7]. Furthermore, compliance rates were lowest at the end of the year in December (60.5%) and in June (62.09%), reflecting a decreased inclination to report into the QA database near the holiday season and at the end of the academic year. These findings may elucidate a pattern in anesthesiology resident behaviors specific to QA database entry throughout the academic year.
Over the 5-year period analyzed, rates of entry into the QA database steadily declined from an initial rate of 84.37% in 2013 to 45.16% in 2017. We suspect that this finding is due to a lack of formalized resident and attending education about the availability and importance of entering cases into the QA database. Hall et al. found that deficient in-service education is a major factor in the incidence of reporting adverse outcomes amongst healthcare providers[8]. Furthermore, it has been previously demonstrated by Vigoda et al. that increased education in the form of formal meetings regarding QA documentation departmental policy coupled with regular announcements at grand round meetings increased QA compliance rates from 48–55%. Moreover, when these investigators added an individualized feedback intervention to inform providers of their case load and compliance rates for the month, compliance rates into the database increased to 78% [4]. Regular feedback with providers to use the voluntary QA incident form was also shown by Haller et al. to be a major contributing factor in achieving their 4 year compliance rates of 85.1% [3]. These other studies shed light on possible interventions that may be effective in increasing QA compliance rates at our institution.
A variety of anesthesiology workflow structures exist to capture quality assurance metrics. While some institutions implement a traditional paper-based Quality Assurance form[7], others have adopted electronic forms that are either voluntary[3] or mandatory. In voluntary reporting systems, providers or external-reviewers can choose whether to report data about an adverse event in the operating room. However, the inconsistency in reporting from such a system leads to compliance rates that are low and ultimately results in ineffective quality improvement interventions[9, 10]. Given the inherent flaws in voluntary reporting, Peterfreund et al. customized their Anesthesia information management systems (AIMS) workflow to mandate the completion of an electronic QA form before the end-time of an anesthesia case could be recorded [5]. In reviewing 55,382 cases over the course of a year after implementation of a mandatory QA recording system, the authors found a sustained increase in the number of adverse events that were reported.
The third approach to capture quality assurance information is through active surveillance of anesthesia related data through an institution’s Anesthesia Information Management System (AIMS). This structure implements the automatic detection of abnormal patient vital signs using pre-determined criteria built into the AIMS. Automatic reporting of incidents within anesthesiology boasts obvious benefits of increased time for providers and an error-free, unbiased identification of adverse events that can be investigated in quality improvement interventions[11, 12]. However, factors such as high perceived costs and low perceived need compared to the available monitoring system have limited the wide-spread implementation of automatic capturing systems[1].
{kind=link}