To the best of our knowledge, this study is the longest follow-up analysis for dynamic variation of weight loss during RT and the associated prognostic value of survival among NPC patients. Results of this present study revealed body weight remained largely unchanged during RT for the first two weeks, and dropped fastest at the sixth week of RT. Further analysis revealed that weight loss ≥ 5% during RT was associated with significantly inferior ten-year DFS, OS, and DMFS for NPC. Additionally, older age and chemotherapy were predictive of greater weight loss for NPC.
Numerous studies have demonstrated that among individuals diagnosed with head and neck cancer, weight loss is correlated with poor prognosis [20, 21], especially among NPC patients [10, 11]. Results from the present study aligned closely with prior studies. There are several potential reasons for these findings. First, critical weight loss may result in loosening of posture fixation, inaccurate radiation field, and significant dosimetric change during IMRT [22]. Second, weight loss potentially causes reduction in treatment tolerance and RT breaks, thus influencing therapeutic efficacy [23, 24]. Third, weight loss is often used as a tool for assessment of newly developed malnutrition, which contributes to weakness in immunity defense mechanism, including phagocyte function, anatomic barriers, cellular and humoral immunity. Therefore, increasing infection susceptibility and reduced response to malignancy [25, 26].
Previous studies reported that weight loss ≥ 5% during RT was associated with poor survival [12, 23]. Our results showed that RWL ≤ -5% was associated with poor DFS, OS, and DMFS, aligning with prior studies. However, Du et al. [11] assessed weight loss during the entire treatment procedure and observed weight loss ≥ 10% was an indicator for likelihood of metastasis and survival. One reason underlying this inconsistency cutoff value of RWL may partly be due to potential selection bias in the study population. Collectively, the impact of weight loss on prognosis of NPC can be determined in the present study. Previous literatures reported approximately 90% local control rates for NPC in the IMRT era [27, 28]. Due to recent advances in RT technology, no observed associated differences in LRRFS between patients in high RWL and low RWL groups were found in the present study. These finding are reasonable as excellent locoregional control is expected for IMRT, therefore actual impact of weight loss on LRRFS would be limited.
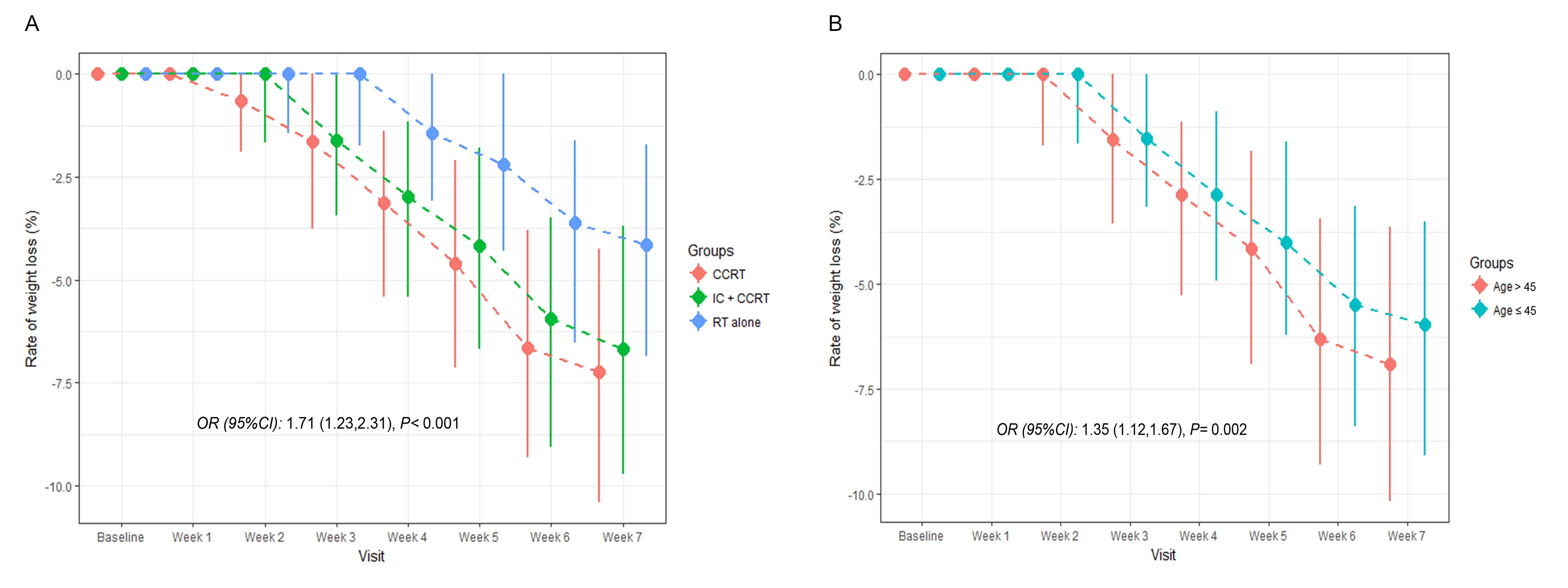
Numerous factors influence weight loss among cancer patients. We observed that patients treated with chemotherapy suffered more weight loss, similar with findings by Qiu et al. [9] and Du et al. [11]. Even with encouraging results attained by multimodal therapy for NPC, acute toxicities are more likely to occur during aggressive chemoradiotherapy [9], including severe oral mucositis, nausea, and vomiting, all directly influencing dietary behavior. Additionally, we observed that patients aged > 60 years had a greater likelihood of suffering higher weight loss. We speculate that elderly patients’ reduced organ reserve, multiple comorbidities, and poor treatment tolerance explain the reason for greater weight loss. Other risk factors including radiation technique, segmentation model, and prescribed dose are partly relevant to oral mucositis and weight loss. Given this research adopts the unified radiation technique, segmentation model, and prescribed dose, we did not include the above factors for analysis.
Since weight loss is common among NPC patients, longitudinal studies assessing weight change over RT time is necessary. This is due to potentially providing a more complete understanding on the relationship between bodyweight and survival among NPC patients. However, prior research primarily evaluated weight loss at a single time point, usually pre- or post-treatment. For this reason, limited knowledge exists about the dynamic change of weight loss during RT. Our results indicated that bodyweight remained generally unchanged in the first two weeks of RT, and then began to drop relatively stable the next three weeks, though fastest in the sixth week of RT. The following reasons may explain the observed results. First, the oral mucous membrane reaction of patients is mild and diet is less affected in the first two weeks of RT. With the increasing number of RT, weight loss is gradually accelerated due to oral mucoiditis, aggravated swallowing pain, and decreased treatment tolerance [4].
There are some limitations that must be noted. First, we lacked detailed information on dietary habit and food intake, as well as data on nutritional status was unavailable for further analysis of weight loss. However, during the study period, no standard criteria for nutritional support in patients undergoing RT has been established. Second, the data used in this study derived from only one institution in an endemic area, where a large proportion of physicians have expertise in diagnosing and treating of NPC compared to other nonendemic areas. Third, we failed to include data regarding other prognostic factors, such as smoking and alcohol consumption status. However, to date, there are no prior studies confirming the role of cigarette smoking or alcohol intake during or after treatment on weight loss. Future studies that incorporate external validation and more diverse data are needed.
{kind=link}