1. Characteristics of the studies and patients included
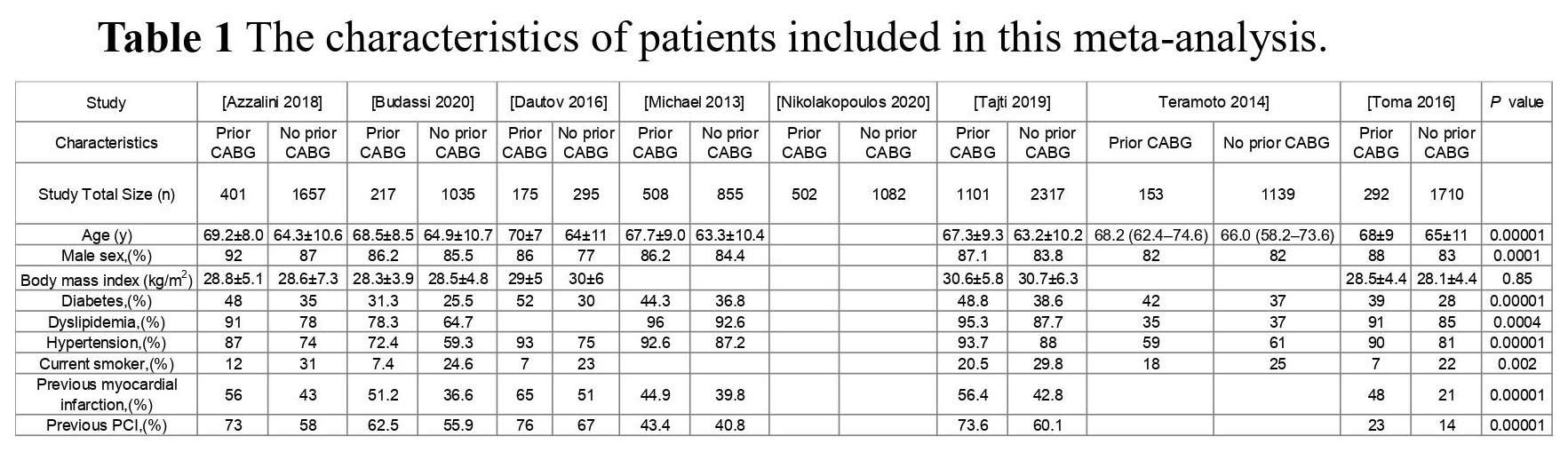
Figure 1 shows the flowchart of the study selection. As a result, a total of 2838 studies were identified through the electronic searches. Then, 2829 studies were excluded after reading the titles and abstracts. The remaining 9 studies were assessed by reading the full texts. Eventually, 8 studies comprising a total of 13439 patients met the inclusion criteria, and were included in qualitative synthesis and meta-analysis[6-12]. The baseline characteristics of the studies included in this meta-analysis are summarized in Tables 1. Out of the 13439 patients enrolled, 3349 (24.9%) presented with previous CABG and 10090 (75.1%) formed the control group for the present analysis. Patients who had undergone CABG were older (68.0±8.8 years vs 64.3±10.3 years; P<0.001), were mostly men(87.2% vs 84.0%; P<0.001), but the BMI had no different (29.6±5.4 vs 29.2±6.0; P=0.85). For past medical history, there were more previous myocardial infarction(54.7% vs 36.7%; P<0.001)and previous PCI (65.7% vs 48.1%; P<0.001). For risk factors, post-CABG patients had a higher prevalence of diabetes mellitus(45.2% vs 33.8%; P<0.001), hypertension(88.3% vs 76.7%; P<0.001)and dyslipidemia(89.4% vs 76.5%; P<0.001),but the current smoking prevalence was lower (13.6% vs 24.5%; P=0.002).
2. Angiographic characteristics
2.1 Lesions location
All studies reported the lesions location, which involved 3422 lesions in post-CABG group and 10430 lesions in no-CABG group. The CTO lesions ratio distributions are shown in Table 2. The right coronary artery (RCA) was the main target vessel in both groups (50.5% vs 48.7%; P=0.49), although, the left circumflex (LCX) was more frequently CTO in the prior CABG group (27.3% vs 18.9%; P<0.01), while left anterior descending artery (LAD) in non-CABG patients (16.0% vs 29.1%; P<0.01).
2.2 Blunt stump
4 studies involving a total of 1914 patients in prior CABG group and 5352 patients in non-CABG patients, reported the incidence of blunt stump in those allocated to pCABG 56.1% (1074 of 1914) or nCABG 44.2% (2367 of 5352) treatment. The pooled outcomes revealed that patients with prior CABG undergoing CTO PCI often have severe blunt stump compared with no-CABG group (OR = 1.71, 95% CI: 1.46-2.00, P<0.001). And low heterogeneity was found among these trials (I2= 40%, P = 0.17; Fig. 2)
2.3 Side branch at proximal entry
Figure 3 pooled analysis of 3 studies from 5208 patients revealed 2507 events (48.1%): per treatment, the event rate was 48.1% (728 of 1513) in the prior CABG group and 48.1% (1779 of 3695) in the non-CABG group. No significant difference was observed between the two groups and the overall OR was 0.88 (95% CI: 0.72-1.07, P=0.21), with moderate heterogeneity (I2 =45%, P=0.16).
2.4 Proximal cap ambiguity
Proximal cap ambiguity in angiographic makes PCI more complex. Only 3 studies involved 5208 participants and 1849 events (35.5%), but a positive result was found. Regarding treatment, 41.5% (628 of 1513) occurred in prior CABG group and 33.0% (1221 of 3695) in non-CABG treated group. The results were OR = 1.45 and 95% CI: 1.28-1.64 (P<0.001), with no heterogeneity (I2 = 0.0%, P = 0.47; Fig. 4)
2.5 Moderate or severe calcifications
A total of 6 studies reported the degree of calcification in both groups, which involved 10905 patients. Figure 2 includes data on the moderate or severe calcifications in both groups. Pooled data analysis revealed 4613 calcification (overall rate 42.3%). Regarding treatment, calcification occurred in 60.0% (1447 of 2412) of prior CABG treated patients and 37.3% (3166 of 8493) of non-CABG treated patients. The overall OR was 2.91 (95% CI: 2.19-3.86, P<0.001), and high degree of heterogeneity was found among these trials (I2 =83%, P<0.001; Fig. 5)
2.6 Bending
Only 3 studies involving a total of 1211 patients reported 4613 bending (overall rate 42.3%) in both groups. Regarding treatment, bending occurred in 53.6% (425 of 793) of prior CABG treated patients and 26.3% (786 of 2987) of non-CABG treated patients. The pooled outcomes revealed the OR was 2.91 (95% CI: 2.19-3.86, P<0.001), and no heterogeneity was found for bending incidence(I2 = 0.0%, P = 0.8; Fig. 6)
2.7 Lesion length
Lesion length > 20 mm have been well recognized as an unfavorable characteristic in angiographic. 4 studies reported this characteristic, which involved 5782 patients and 3553 events in both groups (overall rate 61.4%). Among these patients, 67.8% (736 of 1085) occurred in prior CABG treated group and 60.0% (2817 of 4697) in non-CABG treated group. The pooled outcomes revealed the OR was 1.59 (95% CI: 1.10-2.29, P=0.001), with high heterogeneity (I2 =83%, P<0.001; Fig. 7).
2.8 In-stent CTO
In-stent CTO was reported in 5 studies from 8903 patients and 1242 (overall rate 14.0%) was found. However, no significant difference was found between the two groups: per treatment, the event rate was 14.3% (304 of 2120) in the prior CABG group and 13.8% (938 of 6783) in the non-CABG group. The pooled OR value was 0.99 (95% CI: 0.86-1.14, P=0.88; Fig. 8), and there was no heterogeneity (I2 = 0.0%, P=0.44).
2.9 Lack of interventional collaterals
The outcome occurred in 2013 events among 5208 participants (38.7%) from 3 studies, finding a negative result. Among these patients, 36.8% (557 of 1513) in the prior CABG treated patients and 39.4% (1456 of 3695) in non-CABG treated patients (OR: 0.80, 95% CI: 0.55-1.15, P=0.23), with high heterogeneity (I2 =78%, P=0.01; Fig. 9).
2.10 Inadequate distal landing zone
A total of 7266 patients were included in 4 studies reporting this event. And the incidence was 33.7% (2448 of 7266) in overall rate. Compared with treatment method, 44.1% (844 of 1914) in the prior CABG group and 30.0% (1604 of 5352) in the non-CABG group. The pooled OR value was 1.95 (95% CI: 1.75-2.18, P<0.001; Fig. 10), and there was no heterogeneity (I2 = 0.0%, P=0.54).
2.11 Distal cap at bifurcation
For bifurcation at the distal cap during CTO PCI, only 3 studies were included, reporting 1646 events among 5208 individuals (overall rate 31.6%), but finding a positive result. The incidence was significantly higher in patients with prior CABG (40.0%, 605 of 1513), when compared with non-CABG patients (28.2%, 1041 of 3695). The pooled outcomes revealed the OR was 1.65 (95% CI: 1.46-1.88, P<0.001), with no heterogeneity (I2 = 0.0%, P = 0.49; Fig. 11)
2.12 Previously failed attempt
Previously attempted but failed were more common among harder CTO cases. Five studies provided this data, reporting 1677 events among 8573 individuals (19.6%). Regarding treatment, 18.0% (417 of 2313) occurred in prior CABG group and 20.1% (1260 of 6260) in non-CABG treated group. The pooled outcomes revealed that the rate of previously failed attempt did not vary significantly between two groups (OR: 0.73 [95% CI, 0.48-1.11], P=0.14; I2 = 89%, heterogeneity P<0.001; Fig. 12).
2.13 J-CTO score
Four studies provided data regarding the comparison of J-CTO score between the two groups which involved 7255 patients: 26.3% (1914 of 7255) in the prior CABG group and 73.7% (5352 of 7255) in the non-CABG group. The score was significantly higher in patients with prior CABG, when compared with non-CABG group (2.74±1.24 vs 2.02±1.26; P<0.001). The pooled SMD value was 0.52 (95% CI: 0.42-0.63, P<0.001; Fig. 13), with moderate heterogeneity (I2 =65%, P=0.04).
3. Complication
3.1 Perforation with need for intervention
8544 patients from four studies were included in the analysis of this event and the incidence was 4.24% (362 of 8544) in overall rate. For treatment method, the incidence of perforation was significantly higher in prior CABG patients (5.55%, 124 of 2236), as compared with non-prior CABG patients (3.77%, 238 of 6308). The pooled OR value was 1.91 (95% CI: 1.36-2.69, P<0.001), with lower heterogeneity (I2 = 34%, P = 0.21; Fig. 14)
3.2 Tamponade
A total of 4 studies reported the incidence of tamponade, which involved 7266 participants and 57 events (0.78%). The pooled results indicated that the non-CABG group may have a higher incidence of coronary perforation (0.99%, 53 of 5352), when compared with the prior CABG group (0.21%, 4 of 1914), during the perioperative period of CTO PCI (OR = 0.25, 95% CI 0.09-0.72, P=0.01) with no heterogeneity across studies (I2 = 0.0%, P = 0.64; Fig. 15).
3.3 Major bleeding
A total of 4 studies were included for the major bleeding, which involved 5143 participants and 44 events (0.86%), and no heterogeneity was found for the incidence (I2 = 0.0%, P = 0.67). Furthermore, there was no significant difference between the prior CABG (0.77%, 10 of 1301) and non-CABG group (0.89%, 34 of 3842) regarding major bleeding (OR = 1.18, 95% CI 0.57-2.44, P = 0.65; Fig. 16).
3.4 Contrast-induced nephropathy
Only 20 events among 3780 patients from 3 studies analysis this event and get a positive result. The prior CABG treatment (1.4%, 11 of 793) was significantly associated with higher risks of contrast-induced nephropathy, compared to non-CABG treatment (0.30%, 9 of 2987). And the pooled OR value was 3.40 (95% CI: 1.31-8.78, P=0.001), with no heterogeneity (I2 = 0.0%, P = 0.64; Fig. 17).
{kind=link}
{kind=link}