NLGN2 overexpression is favorable for the survival of breast cancer patients
To determine the prognostic relevance of NLGN2 in breast cancer, we analyzed the survival patterns of the NLGN2hi and NLGN2low groups for each subtype. As shown in Fig. 1A, the NLGN2hi patients had significantly longer overall survival compared to the NLGN2low group (HR, 0.59; 95%CI, 0.5 to 0.69; p < 0.05), including those post-treated (HR, 0.51; 95%CI, 0.41 to 0.64; p < 0.05) (Fig. 1B). The favorable prognostic function of NLGN2 was also confirmed for the basal (HR, 0.72; 95%CI, 0.52 to 1; p < 0.05) (Fig. 1C), luminal A (HR, 0.65; 95%CI, 0.5 to 0.83; p < 0.05) (Fig. 1D), and luminal B (HR, 0.54; 95%CI, 0.39 to 0.73; p < 0.05) (Fig. 1E) subtypes. In contrast, higher expression of NLGN2 was not conductive to the survival of the HER2 + breast cancer patients (HR, 0.59; 95%CI, 0.5 to 0.69; p > 0.05) (Fig. 1F). Taken together, elevated NLGN2 indicates favorable prognosis for breast cancer patients with the basal, luminal A, and luminal B phenotypes.
The prognostic value of NLGN2 for specific molecular subtypes of breast cancer
To further determine the clinical pertinence of NLGN2 in breast cancer, we assessed its prognostic performance in different intrinsic subtypes with or without the estrogen receptor (ER), progesterone receptor (PR) and Erb-B2 receptor tyrosine kinase 2 (HER2) expression. NLGN2 overexpression was not associated with prognosis in the ER negative (-) patients (HR, 0.97; 95%CI, 0.7 to 1.36; p > 0.05) (Fig. 2A) and PR- patients (HR, 1.07; 95%CI, 0.75 to 1.53; p > 0.05) (Fig. 2B), but associated with favorable prognosis in the HER2- patients (HR, 0.7; 95%CI, 0.52 to 0.95; p < 0.05) (Fig. 2C) and not associated with the unfavorable prognosis in ER-/PR-/HER2- patients (HR, 1.18; 95%CI, 0.68 to 2.04; p > 0.05) (Fig. 2D). In addition, there was no significant correlation between NLGN2 and OS in patients with wild type tumor protein p53 (TP53) (HR, 1.46; 95%CI, 0.63 to 3.42; p > 0.05) (Fig. 2E) or mutated TP53 (HR, 0.87; 95%CI, 0.48 to 1.58; p > 0.05) (Fig. 2F). Thus, upregulation of NLGN2 is associated with better prognosis in HER2- breast cancer as opposed to other molecular subtypes.
NLGN2 is favorable in breast cancer patients without lymph node metastasis
Given the relevance of clinical staging and pathological grading in the survival of breast cancer patients, we next analyzed the relationship between NLGN2 expression and the clinicopathological grades. NLGN2 was identified as a favorable prognostic factor in the lymph node non-metastatic (-) patients (HR, 0.65; 95%CI, 0.44 to 0.97; p < 0.05) (Fig. 3A), but not in the lymph node metastatic (+) patients (HR, 0.92; 95%CI, 0.72 to 1.19; p > 0.05) (Fig. 3B). Surprisingly, the expression of NLGN2 was not correlated with the survival of patients diagnosed as Grade 1 (HR, 0.73; 95%CI, 0.25 to 2.1; p > 0.05) (Fig. 3C), Grade 2 (HR, 1.18; 95%CI, 0.71 to 1.97; p > 0.05) (Fig. 3D), and Grade 3 (HR, 0.81; 95%CI, 0.6 to 1.11; p > 0.05) (Fig. 3E). Taken together, NLGN2 correlates to the clinical staging of breast cancer as opposed to pathological grading.
NLGN2 positively correlates with the immunomodulatory signature in breast cancer
Since immune regulation is a key factor in cancer progression, we also analyzed the potential influence of NLGN2 on breast cancer immunity to better understand its prognostic role. Intriguingly, NLGN2 expression was closely related to levels of critical immune effector molecules, including IFNG (Fig. 4A) and GZMB (Fig. 4B). At the cellular landscape, NLGN2 correlated significantly with signatures of crucial subpopulations of tumor-infiltrating lymphocytes [25], including but not limited to cytotoxic T cells (CD3/ CD8) (Fig. 4C), helper T cells (CD3/ CD4) (Fig. 4D), B cells (CD19/ CD20) (Fig. 4E), macrophages (CD14/ CD11b/ HLA-DR) (Fig. 4F), NK cells (CD16/ CD56/ NKG2D) (Fig. 4G), and dendritic cells (CD135/ Flt3/ CD117/ CD26/ CD103) (Fig. 4H). These findings strongly indicate an immune system-dependent role of NLGN2 in breast cancer.
NLGN2 is associated with clinicopathological features and tumor infiltrating CD3 + and CD8 + T lymphocytes in breast cancer
To validate the in silico prognostic data of NLGN2 in breast cancer, we firstly analyzed its in-situ expression levels in fifty in-house patient tissue samples. NLGN2 was highly expressed in 80% (40/50) of the tumor samples, and was significantly associated with larger size, lymph node metastasis, late TNM stage and high histological grade (all p < 0.05), but not with patient age or the expression levels of ER, PR and HER2 (all p > 0.05) (Table 1). Moreover, 84% (42/50) of the samples exhibited high CD3 + T lymphocyte infiltration and 74% (37/50) displayed high CD8 + T lymphocyte infiltration. Furthermore, NLGN2 expression was significantly correlated with the interstitial infiltration of both CD3 + and CD8 + T lymphocytes (both p < 0.01) (Table 2). The representative images of NLGN2, CD3 and CD8 immunohistochemical staining were shown in Fig. 5. These findings further underscore the close association between NLGN2 expression in breast cancer and the clinicopathological features as well as lymphocytes infiltration.
Table 1
The relationship between NLGN2 expression and the clinicopathological features of breast cancer
|
Parameter
|
n
|
NLGN2
|
P value
|
|
Low expression
|
High expression
|
|
Age (years)
|
|
|
|
0.84
|
|
< 50
|
17
|
4(23.5%)
|
13(76.5%)
|
|
|
≥ 50
|
33
|
6(18.2%)
|
27(81.8%)
|
|
|
Tumor size (cm)
|
|
|
|
0.03
|
|
< 5
|
42
|
10(23.8%)
|
32(76.2%)
|
|
|
≥ 5
|
8
|
0(0%)
|
8(100%)
|
|
|
Lymph node metastasis
|
|
|
|
0.03
|
|
+
|
25
|
2(8%)
|
23(92%)
|
|
|
-
|
25
|
8(32%)
|
17(68%)
|
|
|
Grade
|
|
|
|
< 0.01
|
|
I or II
|
26
|
8(30.8%)
|
18(69.2%)
|
|
|
III
|
24
|
2(8.3%)
|
22(91.7%)
|
|
|
Stage
|
|
|
|
< 0.01
|
|
I or II
|
40
|
4(10%)
|
36(90%)
|
|
|
III
|
10
|
6(60%)
|
4(40%)
|
|
|
ER
|
|
|
|
0.07
|
|
+
|
38
|
9(23.7%)
|
29(76.3%)
|
|
|
-
|
12
|
1(8.3%)
|
11(91.7%)
|
|
|
PR
|
|
|
|
0.32
|
|
+
|
35
|
8(22.9%)
|
27(77.1%)
|
|
|
-
|
15
|
2(13.3%)
|
13(86.7%)
|
|
|
HER2
|
|
|
|
0.32
|
|
0 ~ 1 +
|
20
|
5(25%)
|
15(75%)
|
|
|
2 + ~ 3 +
|
30
|
5(16.7%)
|
25(83.3%)
|
|
| ER, PR, and HER2 data were obtained from patients’ pathology records. |
Table 2
The relationship between NLGN2 expression and CD3 + and CD8 + tumor infiltrating lymphocytes
| |
n
|
Tumor infiltrating
CD3 + lymphocyte
|
P
value
|
Tumor infiltrating
CD8 + lymphocyte
|
P
value
|
| |
Low
level
|
High
level
|
Low
level
|
High
level
|
|
NLGN2
|
|
|
|
< 0.01
|
|
|
< 0.01
|
|
Low expression
|
10
|
5(50%)
|
5(50%)
|
8(80%)
|
2(20%)
|
|
High expression
|
40
|
3(7.5%)
|
37(92.5%)
|
5(12.5%)
|
35(87.5%)
|
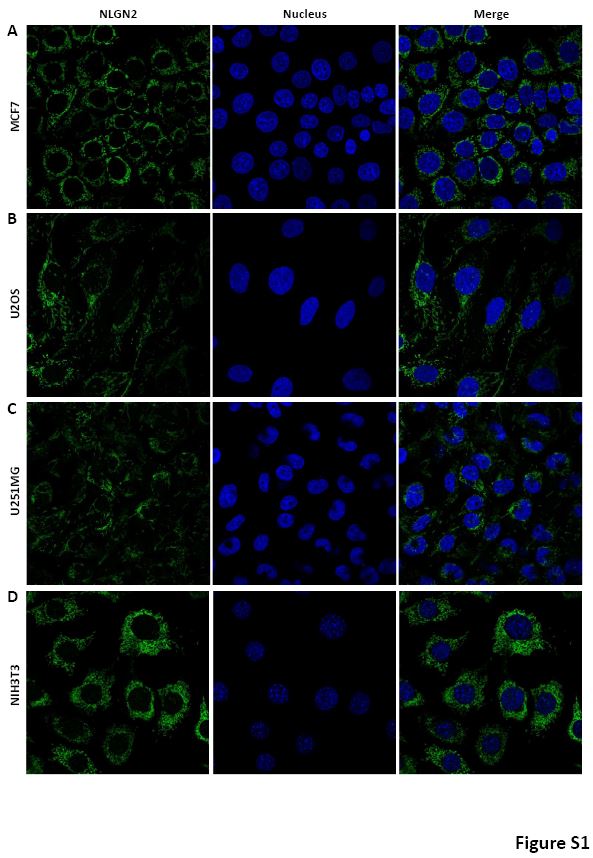
NLGN2 is located in the mitochondria of peripheral breast cancer cells
As shown in Fig. 5, the CD3 + and CD8 + lymphocytes were mainly distributed in the interstitial tissue, but intriguingly, NLGN2 was primarily localized to the cytoplasm rather than the membrane of normal and malignant breast epithelial cells. Given the spatial distribution largely dictates the precise function and mechanism of proteins, more detailed position of NLGN2 was further investigated in breast cancer cells. Interestingly, NLGN2 expression was predominantly localized in the mitochondria of the MCF7 breast cancer cell line (Figure S1A). Moreover, the unusual positioning of NLGN2 in mitochondria was also confirmed in several additional tumor and normal cell lines, including U2OS (Figure S1B), U251MG (Figure S1C), and NIH3T3 (Figure S1D) cell lines. Mitochondrion is a major determinant of cancer cell growth and patient survival due to its pivotal roles in metabolite transport, energy production, apoptosis induction, and the immune stimulation [26]. We therefore hypothesize that the mitochondrial localization of NLGN2 is instrumental to its prognostic role in breast cancer, and should be explored further.
{kind=link}