Results of search
227 studies were identified from our initial search and 146 of them were remained after duplicates removed. 108 of the remained studies were excluded during title and abstract screening. 38 studies were identified for full-text assessment according our inclusion and exclusion criteria and 10 of them were removed because of non-RCT, topical application of TXA or without placebo group. Finally, 28 studies[3,4,8,10-12,14-18,22-38] were included in this meta-analysis. The study selection process is shown in Figure 1
Description of included studies
The characteristics of included studies were shown in Table 1. The 28 included trials[3,4,8,10-12,14-18,22-38] randomized 7446 patients (3712 to tranexamic acid and 3734 to placebo). 14 trials[4,8,11,14-18,24,31,35-38] randomized not less than 100 patients. CABG was conducted in on-pump condition in 17 trails[12,14,16-18,22-25,27,29-31,33,35,37,38], off-pump condition in 9 trails[3,10,11,15,26,28,32,34,36] and both condition in 2 trails[4,8].
Risk of bias within studies
The results of bias risk assessment were showed in Fig 2 A and B. 14 studies[3,11,12,14,16,22-24,26-29,34,37] did not provide a satisfactory description of their random processes. Blinding process was of high risk of bias in one studies[38] and unclear risk of bias in 7 studies[11,12,22-24,28,34] due to unclear description. 3 studies[16,24,30] had unclear or incomplete descriptions of their outcome data. 2 studies[3,35] was considered to be high risk of selective reporting bias because the reported outcome indicators were inconsistent with the planed outcome indicators.
Publication bias
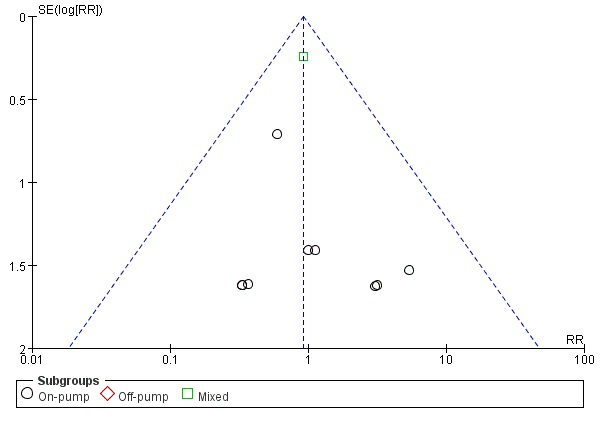
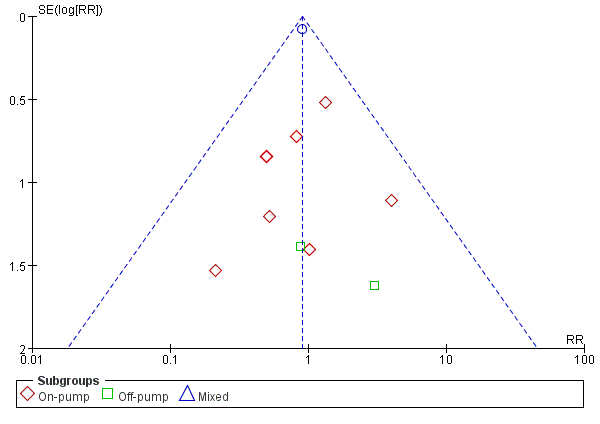
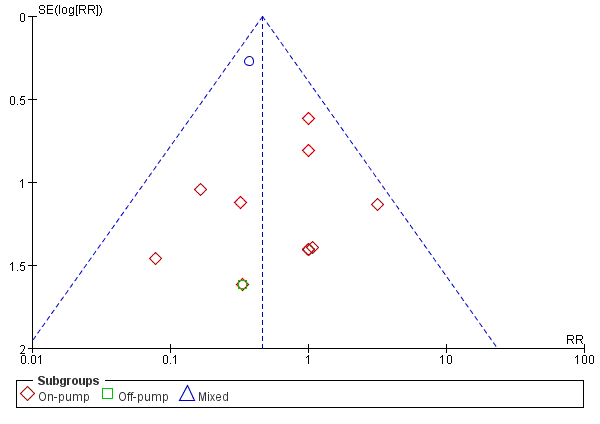
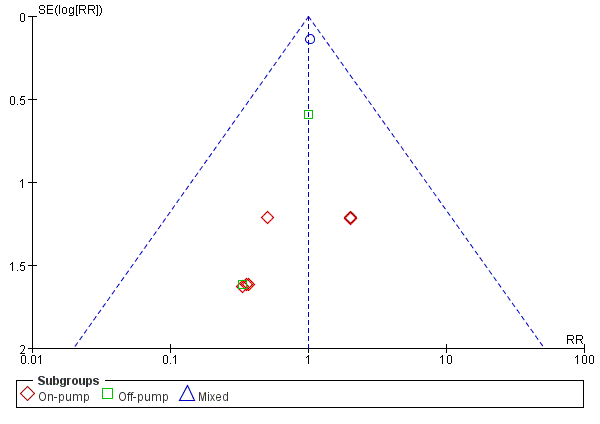
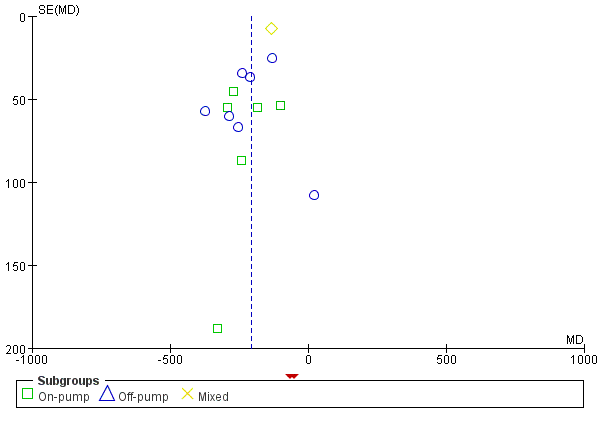
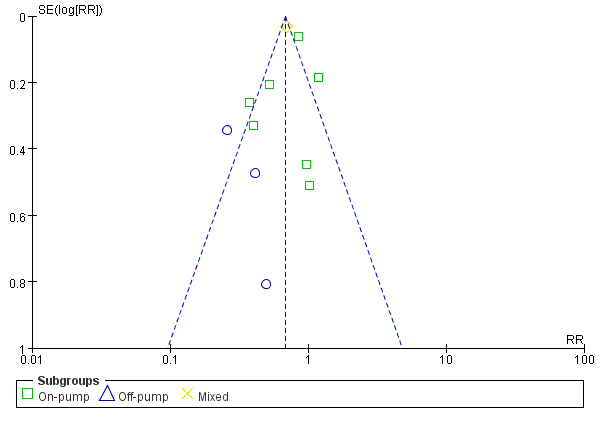
Publication bias was evaluated by funnel plots in the following outcomes: postoperative cerebrovascular accident, reoperation for bleeding, mortality, myocardial infarction, acute renal insufficiency, the frequency of any allogeneic transfusions and 24-hour postoperative chest tube drainage (Supplementary Figs 1-6). All of the plots showed a symmetrical shape suggested low risk of publication bias of the above outcomes.
Quantitative data synthesis
Cerebrovascular accident
There were 22 trials that reported the incidence of postoperative cerebrovascular accident between TXA and placebo, with a total of 6775 participants. TXA did not increase the incidence of cerebrovascular accident overall from meta-analysis [41/3371 vs 45/3404, RR=0.93(0.62-1.39), P for effect=0.71, P for heterogeneity=0.92, I2=0%] (Fig 3).
Sub-analysis in the settings of on-pump CABG with 13 trials included showed no significant increase of cerebrovascular accident incidence in patients who received TXA treatment [9/686 vs 10/711, RR=0.95(0.44-2.06), P for effect=0.90, P for heterogeneity=0.86, I2=0%]. In the setting of off-pump CABG, 8 trails with 749 participants were included and no cerebrovascular accident happened in those trials (Fig 3).
9 studies with a total of 5939 participants were included in the sensitive analysis of studies that randomized not less 100 participants. The conclusion that TXA would not increase cerebrovascular accident incidence was strengthened by the sensitivity analysis [RR=0.87(0.57-1.33), P for effect=0.53, P for heterogeneity=0.95, I2=0%]. Sensitivity analysis that excluded the study with maximum sample size furether strengthened the above conclusion [RR=0.95(0.43-2.10), P for effect=0.90, P for heterogeneity=0.86] (Table 2).
Seizures
In total, 5 studies with 5043 participants reported the incidence of seizures after CABG. The summary RR for postoperative seizures with the use of TXA versus placebo was 5.99 (95% CI 1.77-20.24) which suggested that tranexamic acid would increase the incidence of seizures after CABG (Fig 4).
Reoperation for bleeding
There were 16 trials that reported the incidence of postoperative reoperation for bleeding, with a total of 6259 participants. TXA decreased the incidence of reoperation for postoperative bleeding overall from meta-analysis [35/3125 vs 78/3134, RR=0.46(0.31-0.68), P for effect<0.01, P for heterogeneity=0.63, I2=0%] (Fig 5).
10 studies with 1143 participants were included in the sub-analysis of on-pump CABG, the result of meta-analysis suggested no significant difference of reoperation for postoperative bleeding between TXA and placebo[16/569 vs 26/574, RR=0.64 (0.35-1.15), P for effect=0.14, P for heterogeneity=0.62, I2=0%]. In off-pump subgroup, 4 studies with 384 participants were included and only one patient suffered reoperation in placebo group (Fig 5).
8 trials were included in sensitivity analysis of studies randomized not less than100 patients. The sensitivity analysis supported the result that TXA decreased incidence of reoperation for bleeding in CABG surgery when compared with placebo [29/2812 vs 59/2821, RR= 0.49 (0.32–0.77), P for effect<0.01, P for heterogeneity=0.58, I2=0%]. While sensitivity analysis that excluded the study with maximum sample size did not supported the above conclusion [RR=0.59 (0.34-1.04), P for effect=0.07, P for heterogeneity=0.72] (Table 2).
Mortality
The overall analysis showed that TXA did not significantly decrease the mortality in patients receiving CABG when compared with placebo [33/3196 deaths in the TXA group vs 41/3218 deaths in the placebo group, RR=0.82(0.53–1.28), P for effect=0.38, P for heterogeneity=0.82, I2=0%, with 18 trails included] (Fig 6).
Sub-analysis in the settings of on-pump CABG also showed no statistically significant effect of TXA on mortality [6/639 vs 7/663, RR=0.93 (0.36–2.38), P for effect=0.88, P for heterogeneity=0.62, I2=0%, with 12 trials included]. Sub-analysis in the settings of off-pump included 5 trials, but only one of them reported one patient died in each group (Fig 6).
Sensitivity analysis of studies randomized not less than 100 patients supported the results that TXA did not significantly decrease the mortality in CABG surgery compared with placebo [31/2870 vs 36/2886, RR= 0.87 (0.54–1.40), P for effect=0.56, P for heterogeneity=0.46, I2=0%, with 7 trials included]. The result of sensitivity analysis that excluded the study with maximum sample was consistent with the above analyses [7/875 vs 8/898, RR= 0.93 (0.38-2.27), P for effect=0.88, P for heterogeneity=0.75] (Table 2).
Myocardial infarction
In total, 23 studies with 6714 participants reported the incidence of myocardial infarctions after CABG. The overall analysis showed no increased risk of postoperative myocardial infarction [292/3349 vs 325/3365, RR=0.90 (0.78-1.05), P for effect=0.18, P for heterogeneity=0.89, I2=0%] (Fig 7).
13 studies with 1286 participants were included in the sub-analysis of on-pump CABG, the result of meta-analysis suggested no significant difference of myocardial infarction between TXA and placebo[21/639 vs 24/647, RR=0.9 (0.51-1.58), P for effect=0.71, P for heterogeneity=0.72, I2=0%]. In off-pump subgroup, 9 studies with 798 participants were included, no significant difference of myocardial infarction between TXA and placebo was found neither [2/400 vs 1/398, RR=1.56(0.22-11.23), P for effect=0.66, P for heterogeneity=0.56, I2=0%] (Fig 7).
7 trials were included in sensitivity analysis of studies randomized not less than100 patients. The sensitivity analysis supported the result that TXA did not increase myocardial infarction in CABG surgery when compared with placebo [286/2999 vs 318/3011, RR= 0.90 (0.78–1.05), P for effect=0.18, P for heterogeneity=0.64, I2=0%]. The result of sensitivity analysis that excluded the study with maximum sample was consistent with the above analyses [23/1039 vs 25/1045, RR= 0.94 (0.55-1.61), P for effect=0.81, P for heterogeneity=0.80] (Table 2).
Acute renal insufficiency
There are 14 studies that reported the incidence of acute renal insufficiency in this meta-analysis. The summary RR for acute renal with the use of TXA versus placebo was 1.01 (95% CI 0.77-1.32) which suggested that tranexamic acid would not increase the incidence of acute renal insufficiency (Fig 8).
The summary RR of sub-analysis in the setting of on-pump CABG was 0.91 (95% CI 0.36-2.29) which suggested that TXA did not have adverse effect on postoperative renal function in patients undergoing on-pump CABG. A similar result was found in the sub-analysis in the setting of off-pump CABG [RR=0.85 (0.29-2.47), P for effect=0.76, P for heterogeneity=0.52, I2=0%] (Fig 8).
Sensitivity analysis in trials randomized not less than100 participants reinforced the overall analysis [RR=1.03 (0.79-1.35), P for effect=0.81, P for heterogeneity=0.89, I2=0%, with 7 studies included]. The result of sensitivity analysis that excluded the study with maximum sample was consistent with the above analyses [12/658 vs 14/667, RR= 0.88 (0.42-1.84), P for effect=0.73, P for heterogeneity=0.94] (Table 2).
Transfusion of any blood products
11 trails with a total of 5360 participants reported the postoperative transfusion rate of any blood product. Overall, TXA significantly reduced the transfusion of any blood products [RR=0.64(0.52-0.78), P for effect<0.01, P for heterogeneity<0.01, I2=76%] (Fig 9).
In the subgroup of patients undergoing on-pump CABG, TXA also reduced the transfusion of any blood products, however, this effect was not statistically significant [RR=0.68(0.47-1.00), P for effect=0.05, P for heterogeneity<0.01, I2=81%]. On the other hand, sub-analysis in the setting of off-pump CABG, TXA significantly reduced the transfusion of any blood products [RR=0.32(0.19-0.53), P for effect<0.01, P for heterogeneity=0.60, I2=0%] (Fig 9).
In the sensitivity analysis that included all the studies that randomized not less than 100 participants, TXA significantly decreased the transfusion of any blood products [RR=0.64(0.50-0.81), P for effect<0.01, P for heterogeneity<0.01, I2=86%]. The result of sensitivity analysis that excluded the study with maximum sample further enhanced the above analyses [139/396 vs 216/363, RR= 0.29 (0.20-0.40), P for effect <0.01, P for heterogeneity <0.01] (Table 2).
Postoperative chest tube drainage in the first 24 hours
In total, 16 studies with 6247 participants were included in the meta-analysis of postoperative chest tube drainage in the first 24 hours. One of them[18] divided participants into two groups according to the difference in fluid use and reported the drainage of patients receiving TXA and placebo in both groups separately. We treated these two sets of data as two separate studies in the meta-analysis. Overall, the chest tube drainage was significantly decreased by TXA when compared with placebo [MD=-206.19, 95% CI (-248.23, -164.15), P for effect<0.01, P for heterogeneity<0.01, I2=72%] (Fig 10).
Sub-analysis in the settings of on-pump CABG with 8 trials included showed no significant decrease of chest tube drainage in the first 24 hours in patients who received TXA treatment [MD=-211.36, 95% CI (-263.13, -159.59), P for effect<0.01, P for heterogeneity=0.26, I2=20%]. A similar result was found in the sub-analysis in the setting of off-pump CABG [MD=-220.25, 95% CI (-290.58, -149.91), P for effect<0.01, P for heterogeneity=0.26, I2=76%] (Fig 10).
7 studies with a total of 5674 participants were included in the sensitive analysis. The conclusion that TXA would decrease chest tube drainage in the first 24 hours was strengthened by the sensitivity analysis [MD=-208.30, 95% CI (-274.12, -142.48), P for effect<0.01, P for heterogeneity<0.01, I2=83%]. The sensitivity analysis that excluded the study with maximum sample also supported the above conclusion [MD=-215.42 , 95% CI (-259.48, -171.57), P for effect <0.01, P for heterogeneity<0.01, I2=83%] (Table 2).
Quality of the evidence
The GRADE approach was adopted to evaluate the quality of each outcome and ‘‘Summary of findings’’ tables were presented (Table 3). In general, the overall quality of evidence in the meta-analyses of postoperative seizures and reoperation for bleeding was high. However, the overall quality of evidence in the meta-analyses of postoperative transfusion of any blood products and chest tube drainage in the first 24 hours was very low due to the problems of inconsistency and risk of bias. The overall quality of evidence of other outcomes was moderate due to risk of bias.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}